

The infection due to cytomegalovirus is the most common congenital infection in developed countries, and one of the main causes of psychomotor impairment and neurosensory hearing loss of infectious origin.
The present study has its objectives to describe the clinical-analytical and neuroimaging of patients with secondary neurological sequelae secondary to the congenital cytomegalovirus infection and then compare them with the group of patients with a congenital cytomegalovirus infection that did not have neurological symptoms during their follow-up.
Material and methodsA retrospective, observational, cohort study was conducted that included all the cases of congenital cytomegalovirus infection from 2003 until 2018 and the short-medium term neurological sequelae were evaluated. Prenatal, perinatal, and postnatal data of patients with neurological sequelae were compared against those that did not present with any.
ResultsA total of 60 patients with congenital cytomegalovirus infection were recorded during the study period, with 65% having neurological involvement during their follow-up period (62.2% with psychomotor impairment, 61.5% with microcephaly, 46.2% loss of hearing, 27.8% motor disorders, 20.5% epilepsy, and 5.6% with chorioretinitis). In the patient group that had sequelae, the presence of clinical symptoms during the neonatal period, as well as changes in the neuroimaging study, were the most common, with both being statistically significant compared to the asymptomatic group. The patients with neurological involvement also had a higher score on the Noyola et alneuroimaging scale.
ConclusionsThe symptoms at birth, and certain findings in the neuroimaging, like the changes in the white matter or neuronal migration disorders, could predict neurocognitive sequelae in patients with congenital cytomegalovirus infection.
La infección por citomegalovirus es la infección congénita más frecuente en los países desarrollados y una de las principales causas de retraso psicomotor y sordera neurosensorial de origen infeccioso.
El presente estudio tiene como objetivos: describir las características clínico-analíticas y neuroimagen de los pacientes con secuelas neurológicas secundarias a la infección congénita por citomegalovirus y compararlas con el grupo de pacientes con infección congénita por citomegalovirus que no presentaron clínica neurológica durante su seguimiento.
Material y métodosEstudio de cohortes retrospectivo, observacional. Se incluyeron todos los casos de infección congénita por citomegalovirus desde 2003 hasta 2018 y se evaluaron las secuelas neurológicas a corto-medio plazo. Se compararon datos prenatales, perinatales y postnatales de los pacientes con secuelas neurológicas frente a los que no las presentaron.
ResultadosEn el periodo descrito se registraron 60 pacientes con infección congénita por citomegalovirus, presentando un 65% afectación neurológica durante su periodo de seguimiento (retraso psicomotor 62.2%, microcefalia 61.5%, hipoacusia 46.2%, trastornos motores 27.8%, epilepsia 20.5% y coriorretinitis 5.6%). En el grupo de pacientes que presentó secuelas, la presencia de clínica en el período neonatal así como las alteraciones en el estudio de neuroimagen fueron más frecuentes, siendo ambas estadísticamente significativas respecto al grupo asintomático. Los pacientes con afectación neurológica también presentaron mayor puntuación en la escala de neuroimagen según Noyola et al.
ConclusionesLa sintomatología al nacimiento y ciertos hallazgos en la neuroimagen como la presencia de alteraciones de la sustancia blanca o trastornos de la migración neuronal podrían predecir las secuelas neurocognitivas en los pacientes con infección congénita por citomegalovirus.
Infection by cytomegalovirus (CMV) is the most frequent congenital infection in developed countries, with a prevalence of 0.6%.1 It is the leading cause of non-hereditary sensorineural hearing loss,2 although it can also cause neurologic sequelae, such as motor and cognitive impairment, epilepsy or chorioretinitis.3
The risk of vertical transmission of CMV is higher in case of maternal primary infection compared to relapse or reinfection. While vertical transmission can occur at any point in pregnancy, the probability increases in the third trimester.4,5 However, the sequelae are most severe if the infection occurs in the first trimester.6
Certain antenatal sonographic features are suggestive of CMV infection, such as a foetal echogenic bowel, intrauterine growth restriction, oligohydramnios or polyhydramnios, microcephaly, ventriculomegaly, hepatosplenomegaly, liver or intracranial calcifications, ascites or hydrops fetalis.7
Most congenital CMV infections have an asymptomatic course, but 10% of affected infants have symptoms at birth such as petechiae, jaundice, hepatosplenomegaly, haemolytic anaemia, lethargy, seizures or sepsis-like or pneumonia-like symptoms, and the mortality is 4%.1
The diagnosis can be made prenatally through isolation in viral culture or a positive polymerase chain reaction (PCR) test for detection of CMV in amniotic fluid, or postnatally in the first 3 weeks post birth through a positive result of PCR for detection of CMV in urine or saliva or viral culture of a blood sample.8 The diagnosis after 3 weeks post birth is retrospective, and requires testing of the dried blood spot collected for the neonatal screening tests.9
Neuroimaging abnormalities are found in more than 60% of symptomatic patients and may include intracranial calcifications (usually periventricular), ventriculomegaly, neonatal lenticulostriate vasculopathy, white matter changes, neuronal migration abnormalities, cortical atrophy, periventricular cysts and cerebellar hypoplasia.10–12
Antiviral therapy has been proven to achieve the best hearing and psychomotor development outcomes in patients symptomatic at birth.13,14 Therefore, it is indicated in patients with symptomatic infection and recommended in those with an abnormal newborn hearing screening.15 The selection of the antiviral agent is made based on severity: ganciclovir is reserved for patients with life-threatening disease and valganciclovir for all other patients.3,16
The most important predictors of neurologic sequelae are symptomatic status at birth and abnormal neuroimaging findings in the first month of life.17,18 Active viral replication in the inner ear is a predictor of unfavourable outcome with sensorineural hearing loss.19,20
The aim of the study was to describe the characteristics of patients with a diagnosis of congenital CMV infection and to analyse the association of potential predictors with specific neurologic outcomes in these patients.
Material and methodsWe conducted a retrospective epidemiological and observational cohort study in patients given a diagnosis of congenital CMV infection between January 2003 and December 2018. The study was carried out by the department of paediatric neurology in collaboration with the department of neonatology of the Hospital Universitario y Politécnico La Fe, a tertiary care hospital in the Valencian Community (Spain).
We included patients given a diagnosis of CMV infection within 3 weeks of birth based on a positive PCR test for detection of CMV in blood or urine. We also included patients aged more than 3 weeks with a positive serological test (CMV-specific immunoglobulin M [IgM]) or a positive viral load in the plasma or the dried blood spot obtained for neonatal screening. Urine and blood samples were processed for detection of CMV by means of multiplex real-time PCR or viral culture using the shell vial method.
We considered patients to be symptomatic at birth if any of the following clinical manifestations were present: intrauterine growth restriction (defined as a birth weight below –2 standard deviations [SDs] from the mean), microcephaly (defined as a birth head circumference below –2 SDs from the mean), petechiae, hepatomegaly, splenomegaly, neurologic impairment (hypotonia), sensorineural hearing loss (abnormal result in otoacoustic emissions screen, confirmed by auditory brainstem response), chorioretinitis, thrombocytopenia (<100 000 platelets/µL), elevation of liver enzymes (alanine transferase > 100 U/L; normal range, 10–40 U/L) or cholestasis (direct bilirubin > 3 mg/dL; normal range, 0.1–1.1 mg/dL).3
We collected data on demographic characteristics (sex), prenatal history (maternal infection, drug consumption, findings of antenatal ultrasound examinations and intrauterine growth), perinatal history (gestational age at birth, birth weight) and postnatal variables such as neonatal symptoms and neurologic sequelae, viral load, magnetic resonance imaging (MRI) findings, transfontanellar cranial ultrasound scan findings, and treatment (drug and dosage).
We classified patients based on the presence or absence of neurologic sequelae in the first 2 years of life. We defined neurologic sequelae as presence of sensorineural hearing loss (hearing loss > 20 dB), microcephaly (defined as a head circumference below –2 SDs from the mean), psychomotor retardation (defined as score below –2 SDs in at least 2 psychomotor development scales), intellectual disability, behavioural disorders (including autism spectrum disorder and attention-deficit hyperactivity disorder) or specific language impairment, childhood cerebral palsy (based on the Gross Motor Function Classification System [GMFCS]), chorioretinitis or epilepsy. Group A comprehended patients without neurologic sequelae and Group B patients with neurologic sequelae.
When it came to neuroimaging tests, we assessed patients by means of ultrasound and with 1.5 Tesla MRI. We obtained sagittal, axial and coronal views, and most MRI examinations included FLAIR sequences. The images were interpreted by an experienced paediatric radiologist. We classified the severity of neurologic involvement using the neuroimaging scale developed by Noyola et al. as modified by Alarcón et al.19,21
We performed the statistical analysis with the software SPSS version 19.0; we defined statistical significance as a P-value of less than .05. We have summarised quantitative data as mean and standard deviation and qualitative data as percentages. We used the Shapiro-Wilk test to test the normality assumption and found that the sample followed a non-normal distribution, so we used the Mann-Whitney U test to compare quantitative data and the chi square test or the Fisher exact test to compare qualitative data. We also performed a binary logistic regression analysis with forward selection including all possible predictors (gestational age, history of intrauterine growth restriction, abnormal cranial ultrasound findings, abnormal MRI findings and received treatment).
The study was approved by the Bioethics Committee of our hospital.
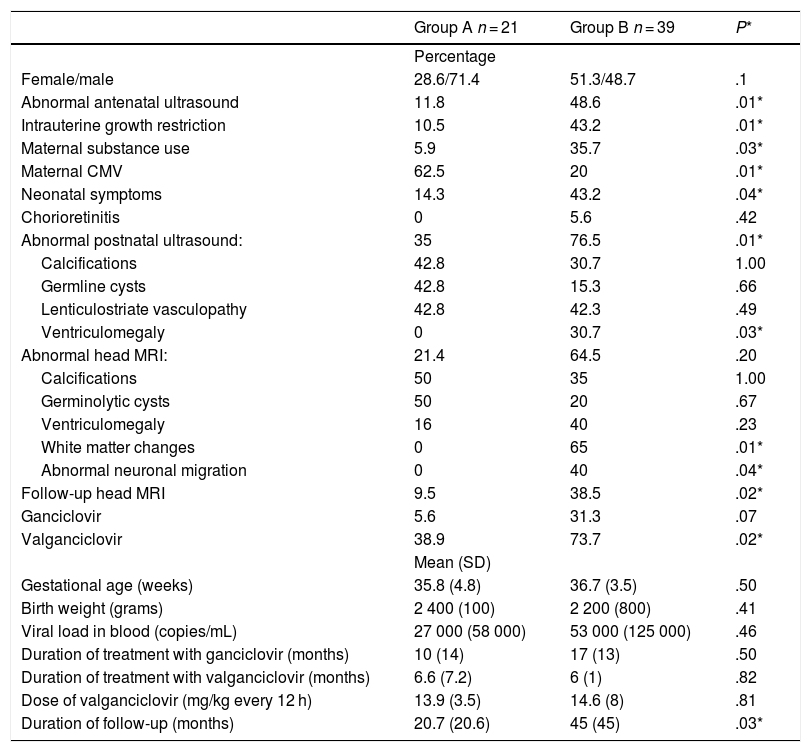
ResultsThe sample included 60 patients with congenital infection by CMV, 21 without neurologic sequelae (35%, group A) and 39 with neurologic sequelae (65%, group B). Table 1 presents the study results.
Comparison of study variables in groups A (without neurologic sequelae) and B (with neurologic sequelae).
| Group A n = 21 | Group B n = 39 | P* | |
|---|---|---|---|
| Percentage | |||
| Female/male | 28.6/71.4 | 51.3/48.7 | .1 |
| Abnormal antenatal ultrasound | 11.8 | 48.6 | .01* |
| Intrauterine growth restriction | 10.5 | 43.2 | .01* |
| Maternal substance use | 5.9 | 35.7 | .03* |
| Maternal CMV | 62.5 | 20 | .01* |
| Neonatal symptoms | 14.3 | 43.2 | .04* |
| Chorioretinitis | 0 | 5.6 | .42 |
| Abnormal postnatal ultrasound: | 35 | 76.5 | .01* |
| Calcifications | 42.8 | 30.7 | 1.00 |
| Germline cysts | 42.8 | 15.3 | .66 |
| Lenticulostriate vasculopathy | 42.8 | 42.3 | .49 |
| Ventriculomegaly | 0 | 30.7 | .03* |
| Abnormal head MRI: | 21.4 | 64.5 | .20 |
| Calcifications | 50 | 35 | 1.00 |
| Germinolytic cysts | 50 | 20 | .67 |
| Ventriculomegaly | 16 | 40 | .23 |
| White matter changes | 0 | 65 | .01* |
| Abnormal neuronal migration | 0 | 40 | .04* |
| Follow-up head MRI | 9.5 | 38.5 | .02* |
| Ganciclovir | 5.6 | 31.3 | .07 |
| Valganciclovir | 38.9 | 73.7 | .02* |
| Mean (SD) | |||
| Gestational age (weeks) | 35.8 (4.8) | 36.7 (3.5) | .50 |
| Birth weight (grams) | 2 400 (100) | 2 200 (800) | .41 |
| Viral load in blood (copies/mL) | 27 000 (58 000) | 53 000 (125 000) | .46 |
| Duration of treatment with ganciclovir (months) | 10 (14) | 17 (13) | .50 |
| Duration of treatment with valganciclovir (months) | 6.6 (7.2) | 6 (1) | .82 |
| Dose of valganciclovir (mg/kg every 12 h) | 13.9 (3.5) | 14.6 (8) | .81 |
| Duration of follow-up (months) | 20.7 (20.6) | 45 (45) | .03* |
The first part of the table presents qualitative data described as percentages and the second part quantitative data summarised as mean and standard deviation.
MRI, magnetic resonance imaging; SD, standard deviation.
As for the prenatal factors under study, 32.1% of patients had a history of intrauterine growth restriction, and abnormalities associated with CMV infection (such as periventricular calcifications or ventriculomegaly) were detected in the antenatal ultrasound scan in 30%. Maternal infection by CMV was diagnosed during pregnancy in 16 cases (34.8%), most frequently in the first trimester. There were also cases of coinfection by vertical transmission of human immunodeficiency virus (HIV) from the mother in 3 infants, although active infection by HIV was not found in any of them. We also found 1 case of coinfection by human papillomavirus.
As for the neonatal factors under study, we found that congenital infection was asymptomatic in a majority of patients in the neonatal period (67.2%). The most frequent symptoms were petechiae and hypotonia. In one case, congenital infection was diagnosed by detection of CMV in the dried blood spot collected for the newborn screening, and in all others the infection was diagnosed within 3 weeks of birth. The mean duration of follow-up at the time of the study was 19 months (SD, 11 months).
As a secondary objective, we compared patients with a diagnosis of congenital CMV infection that developed neurologic sequelae (group B) with patients that did not develop neurologic sequelae (group A).
The neurologic sequelae observed in group B were, in order of decreasing frequency, psychomotor retardation (62.2%), microcephaly (61 > 5%), sensorineural hearing loss (46.2%), childhood cerebral palsy (27.8%): 8 patients with spastic quadriplegia (7 patients with GMFCS level 5 and 1 patient with GMFCS level 3) and 2 with hemiplegia (both with GMFCS level I), epilepsy (20.5%) and chorioretinitis (5.6%).
A perinatal factor that appeared to be relevant was the greater proportion of patients with a history of intrauterine growth restriction in group B (43.2% compared to 10.5% in group A) and the more frequent consumption of substances by the mother in group B, both of which were statistically significant. We should also highlight the statistically significant difference in the proportion of patients with abnormal findings in the antenatal ultrasound (11.8% in group A versus 48.6% in group B). As for the postnatal variables, we found that CMV infection was symptomatic in 14.3% of patients in group A compared to 43.2% in group B, a statistically significant difference.
The first neuroimaging test performed in most patients was the cranial ultrasound, done in 97% of the sample. The sonographic findings were suggestive of CMV infection in 76.5% of patients in group B compared to 35% of patients in group A, a statistically significant difference. The most frequent abnormal sonographic findings in group B were lenticulostriate vasculopathy (42.3%), periventricular calcifications (30.7%), ventriculomegaly (30.7%) and germinolytic cysts (15.3%). Other abnormalities found less frequently included hydranencephaly, intraventricular haemorrhage grade I–III, neuronal migration abnormalities or cerebral atrophy. When we compared each abnormality in isolation, the only statistically significant difference between groups corresponded to the detection of ventriculomegaly.
A head MRI was performed in 77% of patients, detecting abnormalities associated with congenital CMV infection in 56.6% (64.5% of patients in group B compared to 21.4% of patients in group A, although the difference was not statistically significant). These included white matter abnormalities (28.2%), periventricular calcifications (21.7%), ventriculomegaly (19.5%), neuronal migration abnormalities (17.4%) and germinolytic cysts (7%). Of these abnormalities, the only ones present in a significantly greater percentage of patients in group were white matter and neuronal migration abnormalities. A follow-up MRI scan was performed at age 2 years in most of the patients with neurologic sequelae (group A, 9.5%; group B, 38.5%), in which the findings did not differ significantly from those of the initial MRI scan.
The neonatal cranial ultrasound was normal in 10 patients, of who 9 were further evaluated with a head MRI. The findings of MRI were abnormal in 1 of these patients, revealing a neuronal migration abnormality (pachygyria). This patient developed childhood cerebral palsy with level V in the GMFCS, hearing loss, microcephaly and epilepsy. On the other hand, the head MRI was normal in all 5 cases in which the sole abnormal sonographic feature had been lenticulostriate vasculopathy. However, these patients went on to have neurologic sequelae: 2 developed sensorineural hearing loss, 2 had psychomotor retardation and 1 microcephaly. In the subset of patients that developed childhood cerebral palsy, neuroimaging abnormalities did not differ significantly from those found in the rest of the patients with neurologic sequelae. We found a greater percentage with cerebral atrophy (20%) and a greater percentage with neuronal migration abnormalities (77.8%) such as polymicrogyria, pachygyria, lissencephaly and schizencephaly.
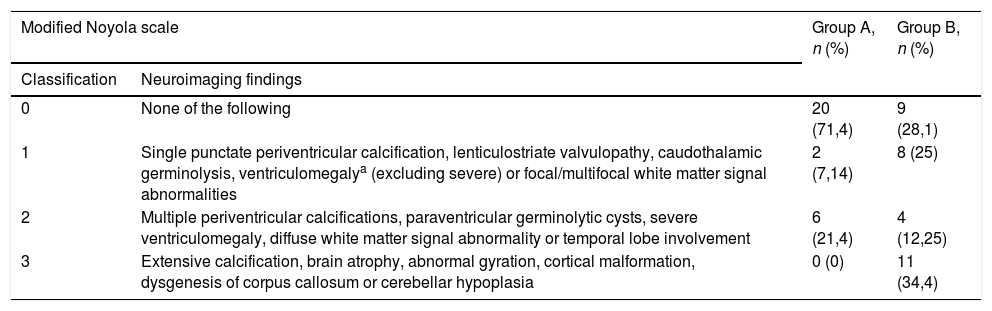
Applying the classification of Noyola et al.19 modified by Alarcón et al.,21 21.4% (6/28) of patients without neurologic sequelae had abnormalities corresponding to a score of 2 and none had abnormalities with a score of 3, and level-0 abnormalities were most frequent in this group (71.4%). On the other hand, as many as 28% of patients with neurologic sequelae had neuroimaging abnormalities corresponding to a score of 0, although abnormalities in this group most frequently corresponded to a score of 3 (34.4%) (Table 2).
Comparison of neuroimaging abnormalities in groups A and B.
| Modified Noyola scale | Group A, n (%) | Group B, n (%) | |
|---|---|---|---|
| Classification | Neuroimaging findings | ||
| 0 | None of the following | 20 (71,4) | 9 (28,1) |
| 1 | Single punctate periventricular calcification, lenticulostriate valvulopathy, caudothalamic germinolysis, ventriculomegalya (excluding severe) or focal/multifocal white matter signal abnormalities | 2 (7,14) | 8 (25) |
| 2 | Multiple periventricular calcifications, paraventricular germinolytic cysts, severe ventriculomegaly, diffuse white matter signal abnormality or temporal lobe involvement | 6 (21,4) | 4 (12,25) |
| 3 | Extensive calcification, brain atrophy, abnormal gyration, cortical malformation, dysgenesis of corpus callosum or cerebellar hypoplasia | 0 (0) | 11 (34,4) |
In the binary logistic regression analysis, none of the variables under study (gestational age, intrauterine growth restriction, abnormalities in cranial ultrasound, abnormalities in MRI or received treatment) was an independent predictor of poor neurodevelopmental outcome.
Lastly, we ought to mention the significant differences we found in the duration of follow-up. The mean duration of follow-up was 45 months in group B (SD, 45) compared to 20.7 months in group A (SD, 20). None of the patients died during the follow-up.
DiscussionBetween 60% and 90% of patients with infection by CMV that were symptomatic at birth and 10%–15% of those that were asymptomatic developed neurologic sequelae ranging from isolated sensorineural hearing loss to intellectual disability or motor deficits.22,23 Due to this clinical variability, it would be interesting to identify potential predictors of long-term neurodevelopmental outcomes. Several studies have analysed the association between abnormalities in neuroimaging tests (cranial ultrasound, cranial computed tomography and head MRI) and the clinical presentation.11,18,24–26
The cranial ultrasound scan is a useful, inexpensive, accessible and harmless technique that allows detection of numerous cranial abnormalities associated with infection by CMV. However, it has limitations when it comes to detecting abnormalities in the cortex, white matter and posterior fossa.11 Therefore, while it has been proposed that a normal ultrasound scan may predict a favourable neurodevelopmental outcome,21 the head MRI performs better for detection of certain abnormalities. In a study by Capretti et al., 8.8% of patients with a normal ultrasound examination had abnormalities in the head MRI, and in 20% the MRI provided additional information relevant to the case.11 In our study, out of the 10 patients with a normal cranial ultrasound, 1 was found to have abnormal neuronal migration (pachygyria) on the head MRI and went on to develop significant neurologic sequelae: childhood cerebral palsy with GMFCS level V, deafness, microcephaly and epilepsy, and 2 developed microcephaly. Therefore, we agree with Capretti et al. that the neonatal head MRI can better predict neurodevelopmental abnormalities compared to cranial ultrasound.11
Certain lesions, such as cortical malformations, ventriculomegaly and hippocampal dysplasia, are associated with poorer neurologic outcomes.18,22 Specifically, Minsun et al. found that polymicrogyria, ventriculomegaly, calcifications and white matter abnormalities were significantly associated with epilepsy and polymicrogyria was significantly associated with psychomotor retardation.26 However, white matter abnormalities in isolation may be confused with delayed myelinization before age 2 years, and there is no evidence of this abnormality being correlated to the long-term neurologic outcome or sensorineural hearing loss.18,22,27,28 In our study, 77% of patients underwent a head MRI scan, and the abnormal features detected most frequently were periventricular calcifications, ventriculomegaly and neuronal migration abnormalities, chiefly polymicrogyria and pachygyria.
Several assessment scales have been developed that use the results of neuroimaging tests. Noyola et al. developed a prognostic scale based on the findings of computed tomography that included the presence of calcifications, ventriculomegaly and atrophy. They found that there was a strong correlation between absence of these abnormalities and a favourable neurodevelopmental outcome.19 When it comes to the use of MRI for assessment of central nervous system involvement in CMV infection, while this technique has some limitations in the detection of cerebral calcifications,11 it is more sensitive in the detection of white matter changes, cortical malformations, periventricular cysts and hippocampal dysplasia, while offering the advantage of not exposing the patient to ionising radiation.17 For these reasons, Alarcón et al. modified the scale developed by Noyola et al. for use in symptomatic patients and included detection of cerebral dysgenesis and white matter signal abnormalities on the head MRI.21 Applying the 0-to-3 scoring system of this scale, we found that in our sample, 28% of patients with neurologic sequelae (including sensorineural hearing loss, psychomotor retardation and epilepsy) had a score of 0, although on the other hand none of the patients that were free of neurologic sequelae had abnormalities corresponding to a score of 3.
To identify risk factors for prediction of behavioural disorders and cognitive impairment in these patients, Inaba et al. assessed the association of the location and volume of white matter lesions with the presence of intellectual disability or autism, and found that a greater white matter lesion volume measured in the head MRI at age greater than 18 months was associated with a lower intellectual quotient, but not with an increased probability of developing autism spectrum disorder.28 In our study, we did not find any patients that had received a diagnosis of autism spectrum disorder during the follow-up.
Microcephaly is the most specific clinical feature for prediction of severe neurologic sequelae.19,24 In the subset of patients that had microcephaly in the study, 54% had psychomotor retardation, 45% sensorineural hearing loss, 25% epilepsy and 29% childhood cerebral palsy.
Based on our findings, early neuroimaging abnormalities and infectious manifestations in the neonatal period can predict neurologic outcomes in these patients, which is consistent with the previous literature. Since antiviral therapy improves hearing outcomes, congenital CMV infection should be ruled out in patients with abnormal hearing screening results.19,20
Our study included both symptomatic and asymptomatic patients and had a sample size of 60 patients, greater compared to other studies. However, it also had limitations. First, it was a retrospective study. Also, a follow-up MRI was only performed after age 2 years in 28% of patients, so it is possible that delayed myelinization was confused with white matter lesions. This was probably due to the absence of an established MRI protocol in the follow-up of these patients. Another limitation was the long-term follow-up of patients without neurologic sequelae, as these patients could develop late sequelae such as learning disorders, behavioural problems, autism spectrum disorder, attention-deficit hyperactivity disorder, language disorders etc. Therefore, performance of a prospective multicentre study with long-term follow-up would be helpful to determine which risk factors contribute to the development of neurologic sequelae in patients with congenital CMV infection. On the other hand, it must be taken into account that most of the scales currently available are qualitative.
ConclusionIn brief, we found that 65% of our patients had neurologic sequelae in association with intrauterine growth restriction, exposure to substances during gestation, the presence of other infections, clinical manifestations of infection in the neonatal period and detection of white matter changes and neuronal migration abnormalities in neuroimaging tests. We ought to highlight that the detection of abnormalities in the head MRI is not necessarily associated with the future presence of neurologic sequelae and vice versa, as only 64% of the subset of patients with neurologic sequelae in the follow-up had abnormalities in the neonatal neuroimaging tests, while as many as 21% of patients without neurologic sequelae had abnormalities on neuroimaging.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: de Juan Gallach A, Alemany Albert M, Marco Hernández AV, Boronat González N, Cernada Badía M, Tomás Vila M. Secuelas neurológicas en pacientes con infección congénita por citomegalovirus. An Pediatr (Barc). 2020;93:111–117.
Previous presentation: This study was presented as an oral communication at the XLI Annual Meeting of the Sociedad Española de Neuropediatría Pediátrica; June, 14–16, 2018; Girona, Spain.
- Documento de manejo clínico del paciente pediátrico con infección por SARS-CoV-2.
(Actualizado el 26 de Noviembre de 2020) - Test de diagnóstico rápido en las consultas de Pediatría de Atención Primaria y Urgencias Pediátricas en la era COVID-19: más que una recomendación
(Actualizado el 21 de septiembre de 2020) - Consenso nacional sobre diagnóstico, estabilización y tratamiento del Síndrome Inflamatorio Multisistémico Pediátrico vinculado a SARS-CoV-2 (SIM-PedS).
(Actualizado el 27 de Julio de 2020) - Recomendaciones para el manejo del recién nacido en relación con la infección por SARS-CoV-2.
(Actualizado el 27 de Mayo de 2020) - Manejo del paciente pediátrico ante sospecha de infección por el nuevo coronavirus SARS-CoV-2 en atención primaria (COVID-19). AEPap-SEIP/AEP-SEPEAP.
(Actualizado el 27 de Abril de 2020) - Propuesta de adaptación de las recomendaciones de reanimación cardiopulmonar pediátrica avanzada a la infección por coronavirus.
(Actualizado el 11 de Abril de 2020)

articles

Anales de Pediatría (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals