

In the metropolitan area of Barcelona, as well as in other Spanish cities, air quality is getting worse by the year. At the same time, projections of temperature and rainfall alert us to future increases in both parameters.1 In this context, studies assessing the influence of climate and air pollution in children, particularly in relation to respiratory diseases, are necessary. A recent systematic review confirmed the association between exposure to air pollutants (particulate matter with diameters >2.5μm [PM2.5] and >10μm [PM10], nitrogen dioxide [NO2] and sulfur dioxide [SO2]) and the risk of hospital admission due to bronchiolitis.2 A study conducted in primary health care centres in Madrid concluded that NO2 levels (particularly those exceeding 40μg/m3) were associated with increases in paediatric respiratory disease.3 To our knowledge, no similar studies have been done in Barcelona.
As a pilot study, we analysed data for 391 patients from the metropolitan area of Barcelona admitted with bronchiolitis to the paediatric intensive care unit of the Hospital Sant Joan de Déu (Esplugues de Llobregat) between 2011 and 2016. We used the postal code of each patient to add the monthly average temperature and humidity values to the database. We also added the value of the air quality index (“Index Català de Qualitat de l’Aire”, ICQA) 10 days before the date of admission (Barcelona City Council website: https://www.barcelona.cat/ca/; ICQA website: http://dtes.gencat.cat/icqa/?elementsComparacio=ICQA_Municipi.e=Setmana).
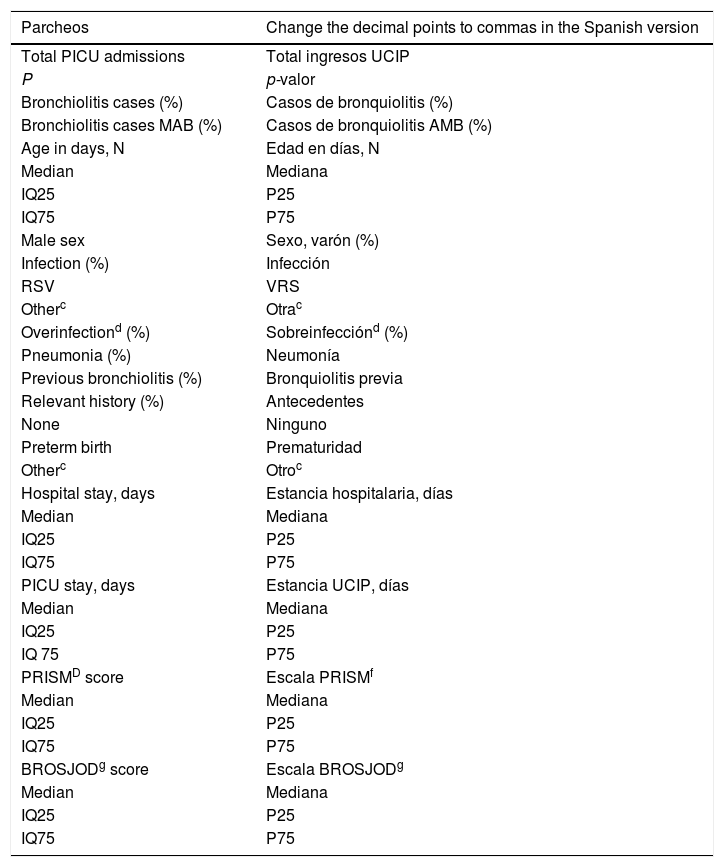
Using the information collected in the database, we found no differences between the years under study in the demographic and clinical characteristics of the patients (Table 1). We conducted time series analyses to identify trends in the number of bronchiolitis cases, temperature and humidity. After adjusting for the effect of seasonality, we found a significant increasing trend in the incidence of bronchiolitis and a significant decreasing trend in the temperature between 2011 and 2016 (Fig. 1). However, the values of adjusted R2 in the regression analyses were less than 10% in both cases. We found no differences in humidity between the years under study.
Total number of patients admitted to the PICU of the Hospital Sant Joan de Déu with bronchiolitis from 2011 to 2016. The clinical and demographic data correspond to patients residing in the metropolitan area of Barcelona (MAB).
| Parcheos | Change the decimal points to commas in the Spanish version |
|---|---|
| Total PICU admissions | Total ingresos UCIP |
| P | p-valor |
| Bronchiolitis cases (%) | Casos de bronquiolitis (%) |
| Bronchiolitis cases MAB (%) | Casos de bronquiolitis AMB (%) |
| Age in days, N | Edad en días, N |
| Median | Mediana |
| IQ25 | P25 |
| IQ75 | P75 |
| Male sex | Sexo, varón (%) |
| Infection (%) | Infección |
| RSV | VRS |
| Otherc | Otrac |
| Overinfectiond (%) | Sobreinfecciónd (%) |
| Pneumonia (%) | Neumonía |
| Previous bronchiolitis (%) | Bronquiolitis previa |
| Relevant history (%) | Antecedentes |
| None | Ninguno |
| Preterm birth | Prematuridad |
| Otherc | Otroc |
| Hospital stay, days | Estancia hospitalaria, días |
| Median | Mediana |
| IQ25 | P25 |
| IQ75 | P75 |
| PICU stay, days | Estancia UCIP, días |
| Median | Mediana |
| IQ25 | P25 |
| IQ 75 | P75 |
| PRISMD score | Escala PRISMf |
| Median | Mediana |
| IQ25 | P25 |
| IQ75 | P75 |
| BROSJODg score | Escala BROSJODg |
| Median | Mediana |
| IQ25 | P25 |
| IQ75 | P75 |
BROSJOD, bronchiolitis severity scale of the Hospital Sant Joan de Déu; PRISM III, Paediatric Risk Score of Mortality III; RSV, respiratory syncytial virus.
a Mann–Whitney U test; bChi square test; cOther: rhinovirus, metapneumovirus, flu, adenovirus, coronavirus, enterovirus, human bocavirus or Bordetella; dHaemophilus and Moraxella; eOther: heart disease, neurologic disease, lung disease or other diseases.

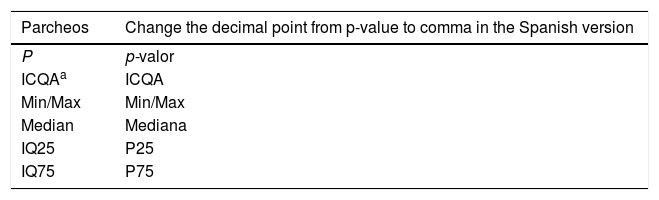
As for the relationship between bronchiolitis and air quality, we observed that the median value of the ICQA on the days with bronchiolitis cases was always within the acceptable range (medians ranging from 50 to 65) with no significant differences between years (Table 2). The median values of the global ICQA in the metropolitan area of Barcelona were similar (medians from 55 to 60) to those observed on the days with cases of bronchiolitis. The pollutant most strongly associated with bronchiolitis cases in the metropolitan area of Barcelona was NO2.
Air quality values on days with bronchiolitis cases from 2011 to 2016.
| Parcheos | Change the decimal point from p-value to comma in the Spanish version |
|---|---|
| P | p-valor |
| ICQAa | ICQA |
| Min/Max | Min/Max |
| Median | Mediana |
| IQ25 | P25 |
| IQ75 | P75 |
The main limitations of this study are the substantial dispersion of cases within the metropolitan area, which posed challenges to the retrieval of environmental data. The heterogeneity found in the databases available for temperature and ICQA, with an insufficient number of weather monitoring stations in some areas and the closure of some stations from 2011 to 2016, have also limited the analyses.
Neither temperature nor pollutants seem to have had an impact on the incidence of bronchiolitis in the metropolitan area of Barcelona from 2011 to 2016. During these years, the city showed sustained pollution levels corresponding to 1.3–1.5 times the recommended limits of the WHO for NO2 and particulates.4 The fact that these pollution levels were sustained over time may explain why our study did not find an association with pollutants, as opposed to the results reported in the United States, where bronchiolitis cases were associated with high values of PM10 due to the presence of steel mills and geographical areas with episodic pollution.5,6 Although we have not detected differences in the distribution of the main pollutants between days with bronchiolitis cases and the rest of the month, it is important to underline that NO2 is the main pollutant present throughout the year in the metropolitan area of Barcelona. This pollutant has already been associated with increased paediatric respiratory disease in Madrid.3 Further studies with larger databases including recent data are needed to understand the relationship between bronchiolitis and the environment.
Please cite this article as: Esteban ME, Bote-González M, Alejandre C, Balaguer M, Jordan I. Influencia de los factores meteorológicos y contaminantes del aire en casos de bronquiolitis grave en el área metropolitana de Barcelona: estudio piloto. An Pediatr (Barc). 2019;92:229–231.
