





Non-specific back pain in children and adolescents has a high prevalence. The aim of this study is to show a Juvenile Back School (JBS) programme and its results in our hospital.
Materials and methodsA total of 139 patients referred to a Juvenile Back School for advice due to pain, deformity or back asymmetry, were included in a prospective observational study. Variables: age, gender, pain, correct postures, sports activities and adherence to JBS and appreciation of these parameters by their parents. Variables were measured with a numerical pain scale and with a survey completed in the first session and 3 months after finishing the JBS.
ResultsA total of 119 patients completed the study (78 female and 41 male). The average was 13.97±2.29 years (9–20). Three months after JBS, the median pain intensity was reduced from 3 to 0 (p<0.0001). There was an improvement in patient postures from 21% to 83% (p<0.0001). Patients did not increase their sport activity after the JBS, although its regular practice was linked with pain improvement after JBS (p<0.02). Performing exercises did not lead to a decrease in pain. There was a poor correlation between parents and children in the evaluation of post-JBS pain.
ConclusionA back school programme could probably contribute to reduce non-specific back pain and improve postural behaviour in young people.
El dolor inespecífico de espalda en niños y adolescentes es muy prevalente. El objetivo de este estudio es presentar un programa de Escuela de espalda juvenil (EDEJ) y sus resultados en nuestro servicio.
Material y métodoEstudio observacional y prospectivo con 139 pacientes, remitidos a la consulta de raquis juvenil por dolor, deformidad o asimetría en la espalda. Variables: edad, sexo, dolor, adopción de posturas correctas, actividad deportiva, adherencia a la EDEJ y percepción de estos parámetros por sus padres. Se midieron las variables mediante una escala numérica del dolor y una encuesta administradas en la primera sesión y a los 3 meses tras la EDEJ.
ResultadosEl estudio fue completado por 119 pacientes (78 mujeres y 41 hombres) con una edad media ± desviación estándar de 13,97±2,29 años (9-20). La mediana de la intensidad del dolor se redujo de 3 a 0 a los 3 meses tras EDEJ (p<0,0001). Aumentaron los pacientes que mejoraron su actitud postural, del 21 al 83% (p<0,0001). No se confirmó un aumento de práctica deportiva post-EDEJ, aunque su práctica habitual se relacionó con una mejoría de dolor post-EDEJ (p<0,02). La realización de los ejercicios no asoció disminución del dolor. Existió mala correlación entre la valoración de padres e hijos sobre el dolor post-EDEJ.
ConclusiónUn programa de escuela de espalda podría contribuir a disminuir el dolor inespecífico de espalda y mejorar los hábitos posturales en jóvenes.
Back pain is one of the most frequent medical problems from the third decade of life. In industrialised countries, between 58% and 84% of adults suffer from it at some point in their lifetimes.1 Back pain has an impact on personal, professional, and socioeconomic levels, as it entails a serious economic burden2 that embraces sick leave, healthcare visits and complementary examinations, treatments, and even worker's compensation and disability.3 Consequently, for some years now efforts have been made to promote back pain prevention at the healthcare and workplace levels, by the development and diffusion of guidelines to prevent low back pain through what we term “Back School”.
But what about children? What is the prevalence of back pain in schoolchildren? And, most importantly, can health professionals or educators prevent it from developing in adulthood?
The data found in the literature shows that the prevalence of non-specific back pain in children and adolescents is almost as high as in adults, ranging between 4.7% and 74.4%,4 although only 24% of these children seek medical attention for their back pain.5 Since there is moderate evidence that back schools are effective in adult patients with recurrent and chronic low back pain in an occupational setting,6 we thought of developing guidelines and exercises for the schoolchildren that visit our offices. This gave rise to what is known as the Juvenile Back School (JBS) in our centre. The aim of this study is to present the JBS and its results in our department.
Materials and methodsWe conducted a prospective observational study at the Hospital Universitario Dr. Peset of Valencia, with patients who were seen for back pain, deformity, or asymmetry in the youth spine clinic of our Rehabilitation department, which were referred for participation in the JBS between April 2010 and April 2011.
We excluded from the study those patients who had a diagnosed back pathology (spinal disc herniation, spondylosis, deformities, etc.) or scoliosis with a Cobb angle >25°.
We gathered data for the following variables: age, sex, pain, severity of pain measured by a numerical scale (NS) ranging from 1 to 10, adoption of correct postures, regular physical activity, adherence to the JBS, and perception of these parameters by the patients’ parents after completion of back school.
Juvenile Back School ProgrammeThe JBS programme comprises three sessions – one informational session and two practise sessions – each lasting 1h, to which the children come accompanied by one adult in the family environment that can overview treatment compliance after the programme.
The informational session is taught by a rehabilitation physician. It is held on the first day and includes basic information on the anatomy and function of the spine, lifestyle measures, the importance of posture, factors involved in back pain, and ergonomic guidelines for the different settings in the child's life (home, school and social environment). The importance of sports activities is discussed, encouraging the practise of sports in a regular and appropriate manner, as well as the transportation of school materials, teaching how to carry the school bag and what the appropriate load is depending on the child's weight. At the end of the session, there is an open discussion to address doubts or concerns, and the attendees are provided with an illustrated handout of the contents (Fig. 1).

The practise sessions are led by physical therapists. At the beginning, they teach children about posture, and the remaining time is devoted to a series of exercises designed to prevent and/or treat dorsal and low back pain by means of stretches and targeted muscle training. The patients are encouraged to perform these exercises regularly at home.
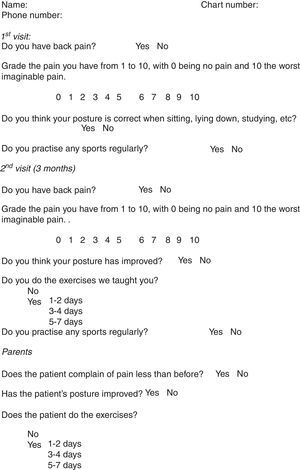
At the same time that we launched the programme, we designed a self-administered survey (Appendix 1). We gave the questionnaire to participants on the first day, before the informational session, asking about the presence or absence of back pain, its intensity, their postural habits, and their physical activity. The second part of the survey was administered at the follow-up visit 3 months after completion of the JBS, repeating the questions about pain, posture, and physical activity, and gathering information on whether participants practised the exercises they were taught, and how often. The second questionnaire also includes some questions for parents to evaluate the correlation between the responses of both generations 3 months after JBS.
Data analysisWe did a descriptive analysis of patient characteristics. To analyse the primary outcome variables, we used the chi-squared test for categorical variables, and Student's t-test and Wilcoxon's test for quantitative variables, depending on the normality of the distribution. We used the kappa coefficient to measure the agreement between observers (parents–children). The level of statistical significance was set at 0.05. We analysed the data using SPSS® version 18.
ResultsA total of 139 patients participated in the JBS during the period under study, of whom 119 completed the programme and the questionnaires. The remaining 20 did not complete the programme for different reasons, detailed in Fig. 2.

Of all participants, 78 were female and 41 male. The mean age±standard deviation was 13.97±2.29 years, with a minimum age of 9 and a maximum of 20.
In the questionnaire administered at the beginning of the programme, 65.5% of patients reported having pain, with a median intensity of 3. Adopting bad postures in daily life activities was reported by 79%. Of all participants, 61.3% reported regularly doing some sports activity in addition to the exercise they did in school (Table 1).
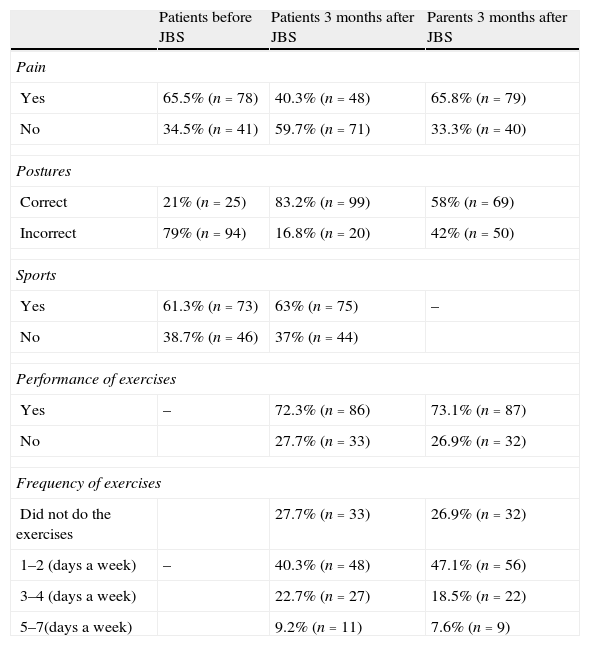
Frequency table for the variables reported by patients before and after the JBS and by parents after the JBS.
| Patients before JBS | Patients 3 months after JBS | Parents 3 months after JBS | |
| Pain | |||
| Yes | 65.5% (n=78) | 40.3% (n=48) | 65.8% (n=79) |
| No | 34.5% (n=41) | 59.7% (n=71) | 33.3% (n=40) |
| Postures | |||
| Correct | 21% (n=25) | 83.2% (n=99) | 58% (n=69) |
| Incorrect | 79% (n=94) | 16.8% (n=20) | 42% (n=50) |
| Sports | |||
| Yes | 61.3% (n=73) | 63% (n=75) | – |
| No | 38.7% (n=46) | 37% (n=44) | |
| Performance of exercises | |||
| Yes | – | 72.3% (n=86) | 73.1% (n=87) |
| No | 27.7% (n=33) | 26.9% (n=32) | |
| Frequency of exercises | |||
| Did not do the exercises | 27.7% (n=33) | 26.9% (n=32) | |
| 1–2 (days a week) | – | 40.3% (n=48) | 47.1% (n=56) |
| 3–4 (days a week) | 22.7% (n=27) | 18.5% (n=22) | |
| 5–7(days a week) | 9.2% (n=11) | 7.6% (n=9) | |
In the check-up done 3 months after completion of JBS we observed a decrease from the initial 65.5% of pain cases (78 cases) to a final percentage of 40.3% (48 cases), a difference that was statistically significant (χ2=15.7; p<0.0001). Pain intensity ratings decreased significantly at 3 months after JBS, changing from a median of 3 to a median of 0 (Wilcoxon test: Z=−5.636; p<0.0001) (Fig. 3).
 before and after JBS.")
However, there was a poor correlation in the pain assessment of parents and children after JBS (kappa coefficient=−0.059±0.081; p>0.05).
We observed improvement in the postures adopted by children in daily activities after participation in the programme, as the number of children that thought they adopted correct postures went from 25 to 99 (from 21% to 83.2%) and those who adopted bad postures decreased from 94 to 20 cases (from 79% to 16.8%) (χ2=92.19; p<0.0001). Parents observed good postural behaviour in their children after JBS, although in a lesser proportion (58%) (χ2=14.236; p<0.0001), resulting in a positive but small correlation (kappa coefficient=0.286±0.77; p<0.0001) with the opinion of the children.
There was no change in relation to the regular practise of sports activities after JBS (χ2=34.178; p<0.0001). The regular practise of sports was not associated to the presence or absence of pain prior to JBS (χ2=0.004; p>0.05); however, it was associated to a lower presence of pain following JBS (χ2=6.12; p<0.02).
Although we observed an overall decrease of pain after JBS training, performing the exercises was not associated to an improvement in pain at 3 months (χ2=0.083; p>0.05). Likewise, when we assessed for the adherence to the exercise schedule (1–2, 3–4 or 5–7 days a week), we observed no correlation between performing the exercises more frequently and decreased pain after programme completion (χ2=2.60; p>0.05) (Fig. 4). We found a high correlation for the reported frequency of exercise performance in parents and children (kappa coefficient=0.60±0.06; p<0.0001).
Discussion
The prevalence of back pain in our sample was 65.5% in the first visit. This figure is slightly higher than figures in other studies for the same age group,7,8 but we have to bear in mind that the population of the study is comprised of patients derived to the Youth Spine Office for a back-related concern, which is often pain, so it is fitting that the number of affected children is greater than in schoolchildren populations that have not undergone any type of selection.
Most of the reviewed studies consistently reported that the presence of back pain increased with age around adolescence, somewhat earlier in girls, possibly at the time that puberty starts, and there is also some evidence that it is more frequent in females than in males.4,5 Kovacs et al.9 performed a study with 7361 schoolchildren ages 13–15 years in Mallorca in which 50.9% of boys and 69.3% of girls reported having had back pain at some time.
In most cases, back pain in children and adolescents is non-specific and tends to resolve itself in a few days even without treatment. However, up to 94% of these children reported that while the pain lasted, it interfered with their daily activities, such as carrying a schoolbag, sitting down at school, or partaking in physical activities.5 In our sample, three months after going through the JBS programme, the number of pain cases and their intensity both decreased. This result has not been observed in most studies on back education in schoolchildren, as they are done in schools and tend to assess what they have learned about the back and posture improvement, but not pain. Only one publication with a control group showed a moderate improvement in the number of medical visits due to back problems in the experimental group,10 and another study that did an analysis over a longer period of time (8 years) did not find any significant differences.11
It is accepted that the risk for back pain in children and adolescents has a multi-factorial nature.12 Some risk factors have to do with lifestyle (overweight, tobacco and alcohol use in adolescents, sedentary lifestyle, muscle capacity, postural habits, etc.); others with school (classroom furniture, competitive sports, carrying books, etc.), and others with medical conditions, such as scoliosis,9 but due to the lack of adequate studies there is no consistent enough evidence to make definitive recommendations. The literature shows a strong association between psychosocial and emotional factors and back pain. It even suggests that they have a greater influence on pain than physical factors.13 Thus, psychological as well as physical symptoms must be assessed to approach the therapeutic management of children or adolescents with back pain.14
Another point of debate is the possible involvement of sports activities, especially competitive sports, as a predisposing factor or risk factor for the development of pain15; however, some sports such as swimming have been identified as preventive factors for the development of back pain in schoolchildren.16 In our study, regular physical activity was not associated with a greater presence of pain at the beginning, but it was at 3 months, a datum that in itself does not suffice to establish definitive conclusions.
One of the most relevant results of our study was the improvement in posture appreciated both by the children subjectively and also by parents. A large percentage of patients reported having improved postures in their daily life activities after the JBS, reaching 83% compared to 21% at the outset. The development and implementation of educational programmes for schoolchildren are supported by studies that, like ours, find an improvement in back posture and knowledge, both at 3 months17 and in the long term in 218 and even 8 years.11 A more controversial aspect is whether a physical exercise programme should be added to the theoretical programme.19 In a study in our area by Mendez and Gomez-Conesa,10 the group that received practical training in exercises had better outcomes than the group that only received theoretical information and a third group that was the control, both in the short-term and at 12 months post-intervention. However, we did not find differences in our sample in the improvement of pain between patients who did the exercises and those who did not.
We want to highlight the disagreement between parents and children in regards to the perceived presence of pain at 3 months, in contrast to their agreement in answers pertaining to correct postures or the frequency in performing the exercises. None of the aforementioned studies included the parents in the educational programmes, so it is not possible to contrast this finding, but it suggests that parents may interpret as pain mild aches that are not that important to their children.
Last of all, we must underscore that the importance of detecting and trying to prevent back pain early in schoolchildren does not reside solely in facilitating their healthy development and increasing their quality of life at the moment, but also in preventing future complications of the same type in the adult population. Various studies have shown that back pain in adolescents is a risk factor for back pain in adulthood,20 and that the risk increases the more the pain experienced during adolescence.21 Acquiring knowledge about the back is the first step towards adopting healthy postural habits to prevent back pain.22
Some of the limitations of this study were the absence of a control group, the small sample size, the short follow-up period, and the bias that could result from selecting the participants in a specialist's office, as they may not be representative of the general population. However, the fact that our results showed improvement in pain and posture habits among our patients encourages us to continue with the JBS and to consider doing more scientifically rigorous studies to confirm these early impressions.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Jordá Llona M, Pérez Bocanegra E, García-Mifsud M, Jimeno Bernad R, Ortiz Hernández R, Castells Ayuso P. Escuela de espalda: una forma sencilla de mejorar el dolor y los hábitos posturales. An Pediatr (Barc). 2014;81:92–98.
