




Diffuse cutaneous mastocytosis (DCM) is the least frequent and most severe form of cutaneous mastocytosis. It is characterised by diffuse mast cell infiltration in the dermis. Its clinical manifestations consist of progressive thickening of the skin, pruritus and systemic involvement due to mast cell degranulation.
Our objective was to review the clinical manifestations and management of cases of DCM in a tertiary care hospital, analysing their diagnosis, treatment, and exacerbations.
Case 1 (Fig. 1a)Male infant aged 4 months with a history of atopic dermatitis and bronchiolitis presenting with recurring urticarial lesions. The patient was referred to the department of paediatric gastroenterology (PGE) for suspected cow's milk protein allergy (CMPA). Nutrition with hydrolysed formula was initiated with no improvement, leading to referral to Dermatology, where the patient received a diagnosis of DCM after undergoing a cutaneous biopsy and laboratory testing (tryptase, 62.4μg/L).

The patient has been treated with H1 and H2 receptor blockers, ketotifen, oral disodium cromoglycate and sessions of psoralen plus ultraviolet A phototherapy (PUVA). He has been admitted to hospital four times and visited the paediatric emergency department (PED) ten times due to exacerbations.
Case 2Male infant aged 6 months, with no history of interest, with repeated episodes of diarrhoea, urticarial rashes and fever. The patient was referred to PGE for suspected CMPA and nutrition with hydrolysed formula was initiated with no improvement. The patient was then referred to Dermatology, where DCM was confirmed by means of skin biopsy, laboratory testing (tryptase, 16μg/L) and a bone marrow biopsy (BMB), which was performed to rule out systemic mastocytosis.
The patient was treated with H1 and H2 receptor blockers, ketotifen, disodium cromoglycate and PUVA. He has been admitted twice and visited the PED three times due to exacerbations.
Case 3 (Fig. 1b)Female newborn aged 13 days, with no history of interest, presenting in the PED with toxic erythema of the newborn and referred to Dermatology, where nodular DCM was diagnosed following a skin biopsy and laboratory testing (tryptase: 13.2μg/l).
The patient is being managed with H1 and H2 receptor blockers, ketotifen and disodium cromoglycate. She has required one admission and six visits to the PED due to exacerbations.
The maintenance treatment of our patients includes antihistamines, ketotifen, oral disodium cromoglycate, environmental measures and PUVA; and during exacerbations, they are treated with systemic corticosteroids and topical disodium cromoglycate.
Two cases have been assessed at the Centro de Estudios de Mastocitosis (Centre for the Study of Mastocytosis [CLMast]), located in the Hospital Virgen del Valle in Toledo (a centre of excellence in the Red Española de Mastocitosis [Spanish Mastocytosis, REMA]).
Diffuse cutaneous mastocytosis consists in a diffuse increase of mast cells in the entire dermis that release the contents of their granules (histamine, tryptase, prostaglandins…) in response to different stimuli, triggering a systemic response: bronchoconstriction, increased permeability, intestinal hypermotility …
The disease manifests with recurrent bullous rashes that result in a characteristic thickening of the skin (“peau d’orange”) and difficult-to-manage pruritus.1 Darier's sign (development of pruritic erythema, wheals or blisters following stroking of lesions due to mast cell degranulation) is pathognomonic,2 and dermographism is a frequent manifestation. Given its large extent, there is systemic involvement with acute episodes of flushing, diarrhoea and bronchospasm. The definitive diagnosis is based on skin biopsy, which evinces elevation of mast cells with perivascular or nodular dermal infiltration. The investigation must be completed with laboratory testing, including serum tryptase level3 (a marker of mast cell activity). Ruling out systemic mastocytosis (systemic symptoms or tryptase >20ng/mL) requires an abdominal ultrasound examination and a BMB.1,3–5 In our patients, the diagnosis was made by means of skin biopsy, and they were referred from Dermatology to Haematology-Oncology for haematological testing, which revealed elevated tryptase levels (mean, 48ng/mL) and a normal sonographic appearance of the abdomen.
There is an index for monitoring the activity of mastocytosis, the SCORMA (SCORing MAstocytosis) index, which assesses the extent (A), intensity (B) and accompanying symptoms (C). Applying the formula A/5+5B+2C/5, a score between 5.2 and 100 is obtained (Fig. 2).
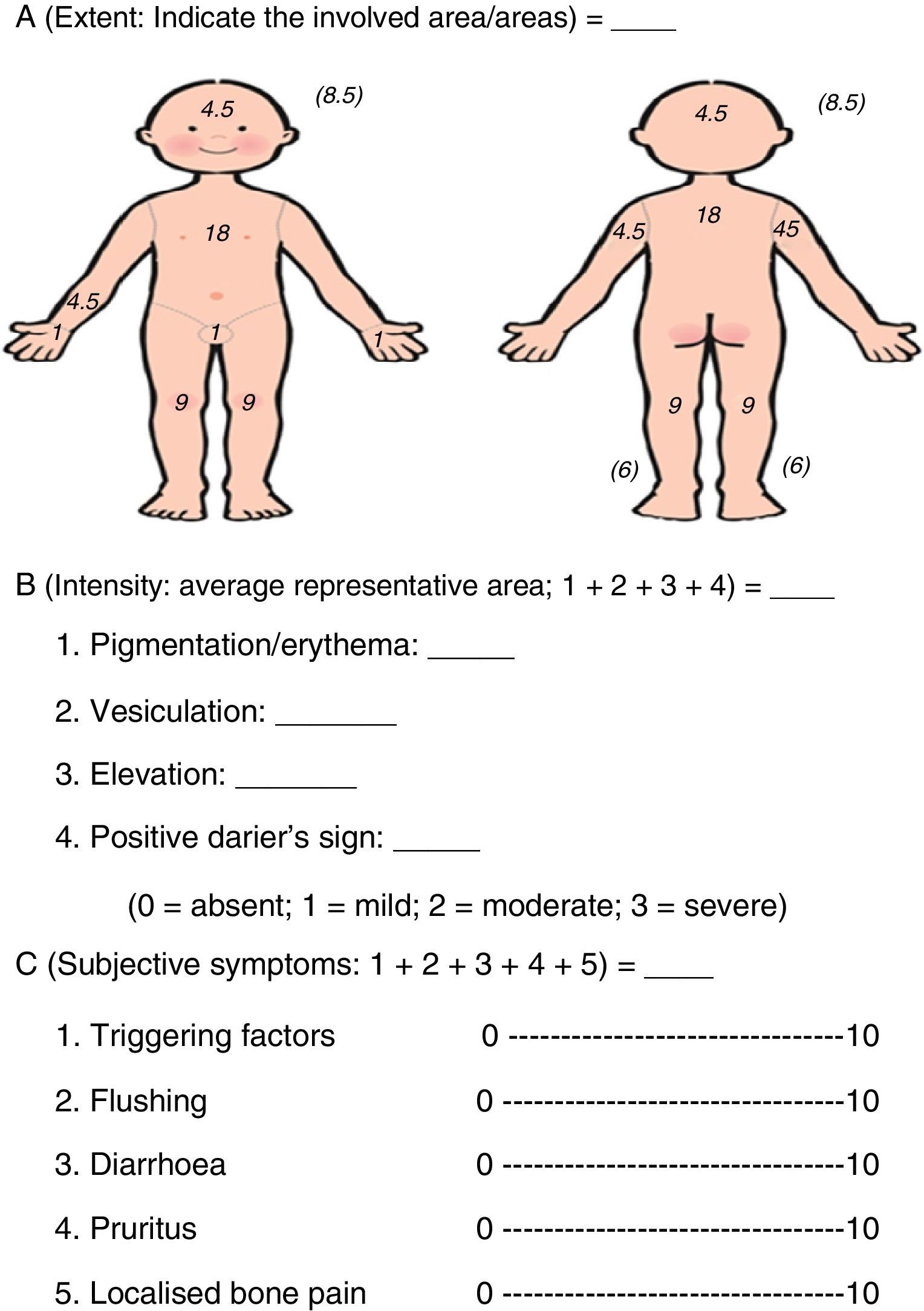
The index is positively correlated with serum tryptase levels, and is useful during exacerbations and for assessing response to treatment. Furthermore, it is less invasive and costly than the determination of tryptase levels.2,4
The treatment is based on:
- 1.
Avoiding factors that trigger the release of granules by mast cells: drugs (aspirin, NSAIDs, opiates, cough medicines, muscle relaxants, thiamine, quinine, aminoglycosides, sympathomimetic and parasympathomimetic drugs), foods rich in histamines or that trigger the release of histamine (chocolate, citrus fruits, shellfish…) and others (fever, exercise, friction…).1
- 2.
Pharmacological treatment: systemic and topical4 agents to control pruritus and achieve a good quality of life. Drugs must be introduced in a stepwise manner: antihistamines, mast cell stabilisers (sodium cromoglycate and ketotifen) and antileukotrienes. Phototherapy with UVB/PUVA can also reduce the number of mast cells.1
At present, there are several areas of pharmacological research, such as c-kit inhibitors, anti-IgE (omalizumab) and interferon alpha.3,6 During acute exacerbations, the dosage of maintenance medications must be increased, adding topical or systemic corticosteroids (1–2mg/kg/day) and topical sodium cromoglycate or antibiotics, if needed.
Patients must be provided with intramuscular adrenaline due to the risk of anaphylactic reactions, and adrenaline auto-injectors are commercially available.4
In conclusion, early diagnosis and a multidisciplinary followup comprising paediatric primary care, dermatology, allergy and haematology/oncology, along with REMA, are needed to improve the management of these patients.
Please cite this article as: Selva Folch B, López Almaraz R, Sánchez González R, Martinez de las Heras B. Mastocitosis cutánea difusa. Presentación de 3 casos y revisión de su manejo terapéutico. An Pediatr (Barc). 2016;84:286–288.
