


Ecthyma gangrenosum (EG) is a cutaneous lesion frequently associated with infection by Pseudomonas aeruginosa.1 It usually affects immunocompromised patients, although its presence is rate at the time of diagnosis of acute lymphoblastic leukaemia (ALL).2 We present 2 cases of EG as the initial manifestation of ALL.
Case 1. Boy aged 19 months, with no history of interest, brought to the emergency department with high fever of 3 days’ duration and a skin lesion measuring 1 × 2 cm with an ulcerated centre surrounded by a necrotic scab in the external surface of the right leg. The salient blood test results were pancytopenia (haemoglobin, 5.2 g/dL; platelet count, 60 000/mm3; neutrophil count, 450 cells/mm3) and a lymphoblast percentage of 78%, suggestive of ALL, with elevation of acute phase reactants (C-reactive protein [CPR], 300 mg/L; procalcitonin [PCT], 33 ng/mL). Broad-spectrum antibiotherapy was initiated with intravenous piperacillin–tazobactam, amikacin and vancomycin following collection of a wound swab and blood sample for culture.
The bone marrow test confirmed the diagnosis of common B-cell ALL with hyperdiploidy. The lumbar puncture was traumatic with cerebrospinal fluid without blasts (CNS 2t). Additional tests (chest radiograph, echocardiography, abdominal ultrasound, cranial magnetic resonance imaging and funduscopic examination) only detected splenomegaly. Remission induction therapy was initiated according to the LAL/SEHOP-PETHEMA-2013 protocol for intermediate risk patients. The patient was reclassified as high risk on day 8 due to poor response to prednisone (>1000 blasts/mm3 in peripheral blood). Multisensitive P. aeruginosa was isolated from the would culture, but the blood culture was negative. Treatment with vancomycin and amikacin was discontinued and the patient completed the 10-day course with piperacillin/tazobactam.
Local treatment started with surgical wound care with application of silver sulfadiazine every 48 h. However, the patient did not respond favourably and required negative pressure wound therapy followed by flap surgery at 40 days post diagnosis. To promote healing of the ecthyma, the patient received treatment with granulocyte colony-stimulating factor (G-CSF) and a healthy-donor granulocyte transfusion.
The outcome was favourable, with a short delay in initiation of chemotherapy. The patient achieved complete remission on day 33, with minimal residual disease (0.01%).
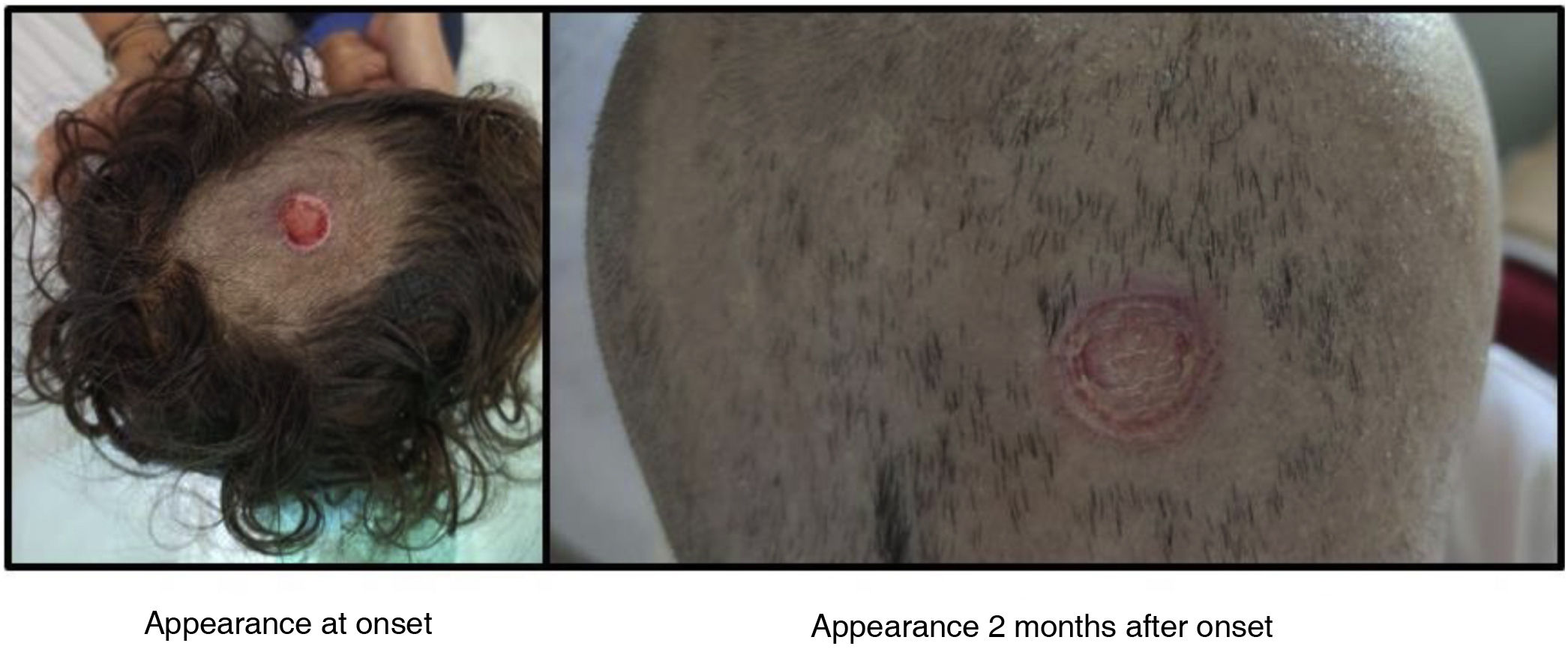
Case 2. Girl aged 3 years, born preterm at 34 weeks’ gestation, brought to the emergency department with high fever of 4 days’ duration and vomiting, decreased feeding, refusal to walk, pallor, asthenia and dizziness. On examination, she appeared septic, with hepatosplenomegaly and an exudative cutaneous lesion measuring 1 × 1 cm in the scalp. Blood tests revealed pancytopenia (haemoglobin, 3.8 g/dL; platelet count, 79 000/mm3; neutrophil count, 0 cells/mm3) and an atypical lymphoblast percentage of 2%, suggestive of an acute lymphoproliferative process, with elevation of acute phase reactants (CPR, 282.7 mg/L; PCT, 18.19 ng/mL) and coagulopathy. Sepsis was suspected, leading to initiation of empiric antibiotherapy with intravenous piperacillin-tazobactam, vancomycin and amikacin following collection of a wound swab and blood sample for culture. The bone marrow test confirmed the diagnosis of acute leukaemia, more specifically, common B-cell ALL with hyperdiploidy. The patient underwent a cranial computed tomography scan and funduscopic examination on an emergency basis, the results of which were normal. The cerebrospinal fluid analysed at 3 days from onset due to coagulopathy and instability associated with sepsis was traumatic but without blasts (CNS 2t). The abdominal ultrasound revealed hepatosplenomegaly; and the results of all other tests were normal.
Remission induction therapy was initiated according to the LAL/SEHOP-PETHEMA-2013 protocol for standard risk patients. Multisensitive P. aeruginosa was isolated from the wound sample, while the blood culture was negative. The patient required wound care every 48 h, administration of G-CSF, enzymatic debridement and negative pressure wound therapy (single-use PICO system), which achieved a favourable response. The assessment of ALL on days 8 and 15 showed improvement. The patient achieved morphological remission on day 33 with minimal residual disease (<0.01%) (Figs. 1 and 2).

The presence of EG in seemingly immunocompetent patients requires an exhaustive investigation to rule out undiagnosed and potentially serious medical conditions, such as the onset of acute leukaemia.1 Cases of EG in patients with ALL during different stages of treatment have been previously described, but none of onset with EG. The characteristic lesion is a purpuric and erythematous macula that rapidly progresses to a haemorrhagic vesicle and eventually to a necrotic ulcer.2 Early treatment with initiation of empiric antibiotherapy is important, as invasive forms of EG are associated with a high mortality.3 Surgical intervention or the use of negative pressure wound therapy is often necessary.4
Furthermore, since neutropenia is one of the main factors involved in its development, the use of G-CSF or granulocyte transfusions may be contemplated with the aim of reducing the duration of neutropenia and expedite wound healing.5
