

To describe the epidemiological characteristics of unintentional injuries due to falls in children under one year and to analyse the risk factors associated with severe injuries.
Patients and methodsThis multicentre, observational and cross-sectional study included all children less than one year treated for unintentional fall in the Emergency Departments of 8 Spanish Hospitals, belonging to the “Unintentional Paediatric Injury Workshop” of the Spanish Paediatric Emergency Society, between March 1st, 2014 and February 28th, 2015.
ResultsOut of 289,887 emergency department cases, 1022 were due to unintentional falls. The median age was 8 months and 52.5% were males. Fall injuries were more frequent among children aged 9–12 months (37.6%), and 83.5% occurred at home. The most common mechanism was fall from nursery equipment (69.4%), and 47.8% occurred from a height under 50cm. More than two-thirds (68%) of falls were witnessed, but in half of the cases (329) the caregiver was not in area. Serious injuries were seen in 12% of cases. In this study, a fall height greater than 50cm, falls in the street, from the arms of the carer, and from the stairs were identified as independent risk factors for worse outcomes.
ConclusionsThe most serious injuries occur in children <3 months and from a height of >50cm, though not related to unwitnessed falls. Because the most common serious injury mechanism is the fall from the arms of the carer, from stairs and falls in the street, these facts should be highlighted in order to avoid morbidity.
Describir las características epidemiológicas de las caídas en menores de un año y analizar los factores de riesgo asociados a las lesiones de mayor gravedad.
Pacientes y métodosEstudio multicéntrico, observacional y transversal, de los niños menores de un año que acudieron por caídas a las Urgencias de 8 hospitales del territorio nacional, pertenecientes al Grupo de Trabajo de Lesiones No Intencionadas de la Sociedad Española de Urgencias de Pediatría, entre el 1 de marzo de 2014 y el 28 de febrero de 2015.
ResultadosDe un total de 289.887 consultas, 1.022 correspondieron a caídas en menores de un año. La mediana de edad fue de 8 meses y el 52,5% fueron varones. Las lesiones por caídas fueron más frecuentes entre los 9 y los 12 meses (37,6%) y en el 83,5% el lugar de caída fue el domicilio habitual. Hasta un 69,4% sufrieron la caída desde dispositivos infantiles y desde una altura inferior a 50cm el 47,8%. En un 68% las caídas fueron presenciadas; sin embargo, en la mitad de los casos (329) el cuidador no se encontraba en el área de alcance. Un 12% de las lesiones fueron graves. En la muestra se identificaron la altura de la caída mayor a 50cm, las caídas en la vía pública, desde los brazos del cuidador y desde las escaleras como factores de gravedad independientes.
ConclusionesLas lesiones más graves se producen en niños <3 meses y desde una altura de >50cm, sin embargo, no se relacionan con caídas no presenciadas. Debido a que el mecanismo más frecuente en las lesiones graves es la caída desde los brazos del cuidador, desde las escaleras y en la vía pública, debemos alertar sobre este hecho para evitar la morbilidad asociada.
In Spain, falls are the leading cause of unintentional injury in children aged less than 14 years, and based on a study on accidents carried out by the Asociación Española de Pediatría de Atención Primaria (Spanish Association of Primary Care Paediatrics) in 2014, they are much more frequent than poisonings or burns.1
Although most instances do not result in serious injuries,2 they constitute the third leading cause of death by unintentional injury in children aged 0–9 years in countries of the European Union, according to the European Child Safety Alliance.3
Infants aged less than 1 year are particularly at risk of suffering fall-related injuries due to their increasing independent mobility and interest in exploring their surroundings,4 resulting in more than one million visits a year to emergency departments in the United States, according to data from the Centres for Disease Control and Prevention (CDC) for the 2000–2006 period.5
Previous studies have emphasised the need to analyse patterns of unintentional injury in the paediatric population within narrower age ranges.6
In Spain, no studies have been conducted to analyse fall-related injuries in infants aged less than 1 year that would help develop preventive strategies targeting this age group.
Numerous preventive strategies have been developed by different governmental agencies,7,8 in spite of which there is evidence that parents are unaware of the mechanisms that lead to fall-related injuries, which hinders effective prevention.
The aim of our study was to describe the epidemiologic characteristics of falls in children aged less than 1 year and to analyse the risk factors or circumstances associated with serious injuries.
Materials and methodsWe conducted a cross-sectional, observational descriptive and inferential multicentric study that included children aged less than 1 year that sought care following a fall in the emergency departments of eight Spanish hospitals members of the Working Group on Unintentional Injuries of the Sociedad Española de Urgencias de Pediatría (Spanish Society of Paediatric Emergency Medicine). The study was approved by the Clinical Research and Ethics Committee of each participating hospital.
We defined fall as the event or effect of falling until hitting ground or a firm surface that stops it. We defined serious injuries as those resulting in fractures or requiring a computerised tomography (CT) scan, interventions such as haemodynamic stabilisation, immobilisation/motion restriction or major surgery, or hospital admission.
Patients were recruited over a period of 12 months between March 1, 2014 and February 28, 2015.
We collected data for epidemiologic variables (age, sex, personal history and motor milestones achieved); the circumstances of the injury (day of the week, setting and mechanism of the fall, witnesses of the fall, type of surface that broke fall and height of fall) and the severity factors defined above (presence and type of fracture, performance of CT scan, need for haemodynamic stabilisation, major surgery or immobilisation/motion restriction or hospital admission). We also documented the incidence of death in the first 24h following the fall. We classified patients into four groups by age (<3 months, 3–6 months, 6–9 months and 9–12 months) based on differences in independent mobility and psychomotor development.
The epidemiologic data were obtained by interviewing parents during the time spent in the emergency department, and collected on a form. Data on severity factors was obtained by reviewing medical records.
The data were reported through an electronic database (Google Drive), the access to which was restricted to the principal investigator of the study.
We analysed the data with the software SPSS 18.0. We performed a descriptive analysis calculating the mean, median and standard deviation for quantitative variables and percentages for qualitative variables. We also performed an inferential analysis using logistic regression. We defined statistical significance as a p-value of less than 0.05 in the tests.
ResultsEpidemiologic dataDuring the period under study, the participating hospitals received a total of 289,887 visits to their emergency departments, out of which we identified 1022 patients aged less than 1 year (0.35%) that had sought care for falls.
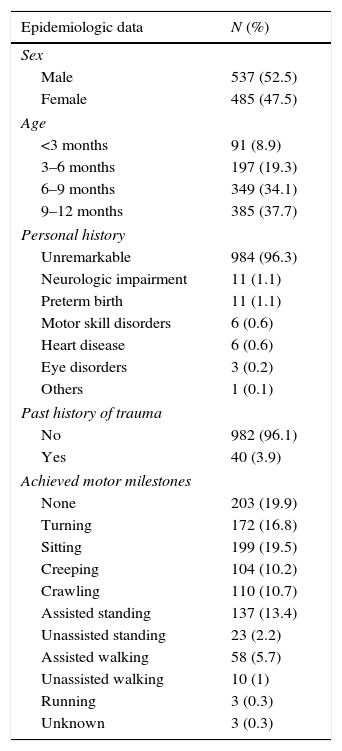
The median age was 8 months, and 52.5% of the patients were male (n=537). Most patients did not have a previous history of trauma (982; 96.1%). The most frequent issues in patients with a relevant previous history were neurologic impairment (11; 1.1%) and preterm birth (11; 1.1%), although most patients did not have a relevant history (984; 96.3%).
Fall-related injuries were most frequent in patients aged 9–12 months (385; 37.7%), followed by patients aged 6–9 months (349; 34.1%). We ought to note that 19.9% of injuries (203) occurred in patients that had not achieved any motor milestones. Table 1 summarises the epidemiologic data.
Epidemiologic data.
| Epidemiologic data | N (%) |
|---|---|
| Sex | |
| Male | 537 (52.5) |
| Female | 485 (47.5) |
| Age | |
| <3 months | 91 (8.9) |
| 3–6 months | 197 (19.3) |
| 6–9 months | 349 (34.1) |
| 9–12 months | 385 (37.7) |
| Personal history | |
| Unremarkable | 984 (96.3) |
| Neurologic impairment | 11 (1.1) |
| Preterm birth | 11 (1.1) |
| Motor skill disorders | 6 (0.6) |
| Heart disease | 6 (0.6) |
| Eye disorders | 3 (0.2) |
| Others | 1 (0.1) |
| Past history of trauma | |
| No | 982 (96.1) |
| Yes | 40 (3.9) |
| Achieved motor milestones | |
| None | 203 (19.9) |
| Turning | 172 (16.8) |
| Sitting | 199 (19.5) |
| Creeping | 104 (10.2) |
| Crawling | 110 (10.7) |
| Assisted standing | 137 (13.4) |
| Unassisted standing | 23 (2.2) |
| Assisted walking | 58 (5.7) |
| Unassisted walking | 10 (1) |
| Running | 3 (0.3) |
| Unknown | 3 (0.3) |
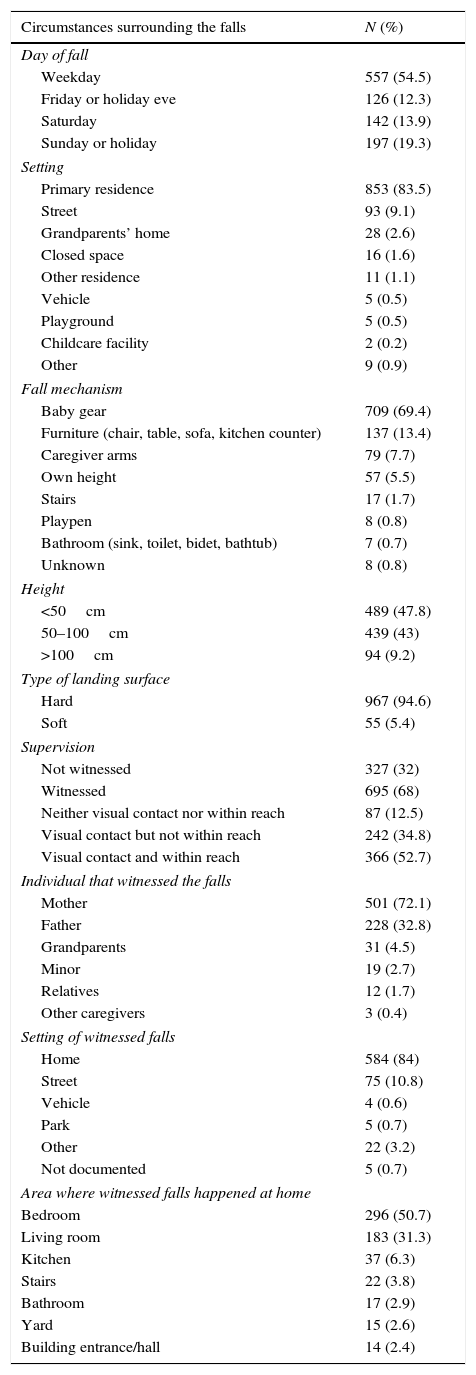
Most falls took place during weekdays (557; 54.5%), while 197 (19.3%) took place on Sundays or holidays (Table 2).
Circumstances surrounding the falls.
| Circumstances surrounding the falls | N (%) |
|---|---|
| Day of fall | |
| Weekday | 557 (54.5) |
| Friday or holiday eve | 126 (12.3) |
| Saturday | 142 (13.9) |
| Sunday or holiday | 197 (19.3) |
| Setting | |
| Primary residence | 853 (83.5) |
| Street | 93 (9.1) |
| Grandparents’ home | 28 (2.6) |
| Closed space | 16 (1.6) |
| Other residence | 11 (1.1) |
| Vehicle | 5 (0.5) |
| Playground | 5 (0.5) |
| Childcare facility | 2 (0.2) |
| Other | 9 (0.9) |
| Fall mechanism | |
| Baby gear | 709 (69.4) |
| Furniture (chair, table, sofa, kitchen counter) | 137 (13.4) |
| Caregiver arms | 79 (7.7) |
| Own height | 57 (5.5) |
| Stairs | 17 (1.7) |
| Playpen | 8 (0.8) |
| Bathroom (sink, toilet, bidet, bathtub) | 7 (0.7) |
| Unknown | 8 (0.8) |
| Height | |
| <50cm | 489 (47.8) |
| 50–100cm | 439 (43) |
| >100cm | 94 (9.2) |
| Type of landing surface | |
| Hard | 967 (94.6) |
| Soft | 55 (5.4) |
| Supervision | |
| Not witnessed | 327 (32) |
| Witnessed | 695 (68) |
| Neither visual contact nor within reach | 87 (12.5) |
| Visual contact but not within reach | 242 (34.8) |
| Visual contact and within reach | 366 (52.7) |
| Individual that witnessed the falls | |
| Mother | 501 (72.1) |
| Father | 228 (32.8) |
| Grandparents | 31 (4.5) |
| Minor | 19 (2.7) |
| Relatives | 12 (1.7) |
| Other caregivers | 3 (0.4) |
| Setting of witnessed falls | |
| Home | 584 (84) |
| Street | 75 (10.8) |
| Vehicle | 4 (0.6) |
| Park | 5 (0.7) |
| Other | 22 (3.2) |
| Not documented | 5 (0.7) |
| Area where witnessed falls happened at home | |
| Bedroom | 296 (50.7) |
| Living room | 183 (31.3) |
| Kitchen | 37 (6.3) |
| Stairs | 22 (3.8) |
| Bathroom | 17 (2.9) |
| Yard | 15 (2.6) |
| Building entrance/hall | 14 (2.4) |
The primary residence (853; 83.5%) was the most frequent setting of falls, and most of the falls witnessed in the home setting took place in the bedroom (296; 50.7%) or the living room (183; 31.3%).
In 69.4% of patients (709), the fall took place from some type of baby equipment, such as strollers, beds, cribs, high chairs or changing stations, and the groups at highest risk of falling from such equipment were infants aged 6–9 months (Fig. 1) (OR, 2.128; 95% CI, 1.302–3.478), infants that had not reach the milestone of standing with support (OR, 1.879; 95% CI, 1.118–3.155) and unwitnessed falls (OR, 2.606; 95% CI, 1.890–3.594).

Although most patients fell from heights of less than 50cm (489; 47.8%), it is worth noting that 9.2% of falls were from heights of more than 1m.
The fall was witnessed in 68% of cases (695), most frequently by the mother (501; 72.1%). However, in half of the cases (329; 47.3%) the caregiver was not within reach of the child to prevent the fall.
Twelve percent of the fall-related injuries (123) were serious. Ninety-four patients had fractures (9.2%), most frequently of the skull (72; 7.1%) followed by long bone fractures (12; 1.2%) and clavicle fractures (10; 1%). Of the 1022 patients treated for fall-related injuries in the emergency departments, 78 (7.6%) underwent a head CT scan, 19 (1.9%) required immobilisation/motion restriction, four (0.4%) required haemodynamic stabilisation, and 2 (0.2%) major surgery. Six percent were admitted to hospital, and no deaths occur in the first 24h following the fall.
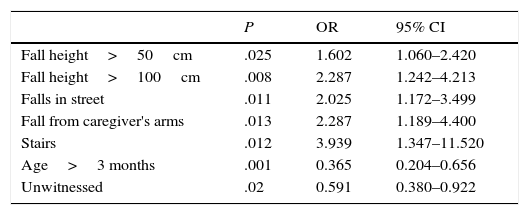
Risk factors for serious injury in falls in children aged less than 1 yearWe performed logistic regression to identify risk factors for serious injury based on the pre-established definition. We identified the height of the fall as an independent risk factor for serious injury, with an OR of 1.602 (95% CI, 1.060–2.420) for fall heights between 50 and 100cm and an OR of 2.287 (95% CI, 1.242–4.213) for heights of more than 100cm. We also found an association between serious injury and falls in the street (OR, 2.025; 95% CI, 1.172–3.499), falls from the caregiver's arms (OR, 2.287; 95% CI, 1.189–4.400) and falls from stairs (OR, 3.939; 95% CI, 1.347–11.520).
On the other hand, we found that age greater than 3 months was a protective factor against serious injury, with an OR of 0.365 (95% CI, 0.204–0.656), and that unwitnessed falls were not associated with greater severity (OR, 0.591; 95% CI, 0.380–0.922) (Table 3).
Logistic regression analysis. Risk factors for serious injury from falls in children aged less than 1 year.
| P | OR | 95% CI | |
|---|---|---|---|
| Fall height>50cm | .025 | 1.602 | 1.060–2.420 |
| Fall height>100cm | .008 | 2.287 | 1.242–4.213 |
| Falls in street | .011 | 2.025 | 1.172–3.499 |
| Fall from caregiver's arms | .013 | 2.287 | 1.189–4.400 |
| Stairs | .012 | 3.939 | 1.347–11.520 |
| Age>3 months | .001 | 0.365 | 0.204–0.656 |
| Unwitnessed | .02 | 0.591 | 0.380–0.922 |
Falls are the most frequent cause of mild unintentional injuries in children and adolescents both in the United States and in Spain,1 and they are a major reason for seeking emergency care,3,5 especially in children aged less than 2 years.1,9 In the United States, falls were the main cause of trauma in infants aged less than 1 year between 2001 and 2006, with an incidence of 3049 per 100,000 inhabitants.5 Identifying the risk factors and circumstances that promote falls is essential for the purpose of establishing effective preventive measures.2,10 Some studies have highlighted the ignorance of parents as to the mechanisms of these falls, which hinders their prevention.
Our study found a prevalence of falls in children aged less than 1 year of 0.35%.
In Spain, the prevalence of falls treated in paediatric emergency departments is higher than that of poisonings,11,12 drownings,13 bicycle falls14 or being hit by motor vehicles.15
It should be taken into account that so far no studies have analysed fall-related injuries in children aged less than 1 year in Spain.
As happened in other case series,2,5,16–18 we found a slight predominance of males, although it was not statistically significant.
In our sample, falls occurred mostly between ages 9 and 12 months and from baby equipment, followed by falls from furniture. Pickett et al. also observed a higher risk of falling between ages 9 and 11 months, although the most frequent mechanism identified in their study was falling from furniture.17 Pitone et al. also highlighted falls from objects as the most common type, with a higher incidence than falls from stairs or from the child's own height.19 However, most studies have not analysed falls from baby equipment as a possible mechanism, which is important given the greater risk of falling when children are left or changed in surfaces at a certain height.16,20
The analysis by age group of Pickett et al. found that infants aged less than 3 months mostly fell from their parents’ arms, while in our sample the main mechanism was falling from baby equipment, followed by falling from the caregiver's arms.17
Few patients in our series had a past history of trauma (3.9%), a percentage that was much lower than those reported in other studies, in which up to 39.7% had a past history of falls.2 This may be explained by the younger age of the sample in our study.
A salient finding was that 19.9% of falls occurred in infants that had not even developed the skill of rolling over, with 8.9% of falls involving infants aged less than 3 months. Other authors have also emphasised that a considerable percentage of falls occur in the early stages of development, a fact that caregivers may not be aware of.2
As was the case in the study conducted by the Asociación Española de Pediatría de Atención Primaria (Spanish Association of Primary Care Paediatrics) on unintentional injuries in the paediatric population of Spain,1 one-third of the falls took place on a Saturday, Sunday or holiday, which may be surprising considering that parents presumably spend more time with their children on these days.
Consistent with the findings of other studies, most of the falls (83.5%) in infants aged less than 1 year took place in the primary residence.5,17 This suggests that most of the injuries in this age group could be prevented by the use of appropriate child restraint and surveillance systems.
We found that 52.2% of the children in our study fell from heights of more than 50cm and identified falls from heights of more of 50cm as a risk factor for serious injury. However, other studies found a height threshold for serious injury of 137cm2 and, in less recent studies, of 150cm.21,22
One-third of the falls were not witnessed by the caregiver (32%), but we ought to note that in nearly half of witnessed falls, the child was not within reach of the caregiver (47.3%), which precluded preventing the fall in a very high percentage of cases (79.3%). However, we did not find an association between unwitnessed falls and increased injury severity. We did not find previous studies in the medical literature that analysed the caregiver's proximity at the time of the fall.
Although most of the injuries observed were mild, 12% of injuries were serious, and 9.1% resulted in fractures, and the risk factors for serious injuries identified in our study were the height of the fall, especially for heights of more than 100cm, and age less than 3 months.
In our study, falls in the street and from the caregiver's arms were also associated with serious injury. However, no previous studies have shown an association between these factors and serious injury.
We also found that falls from stairs were associated with serious injuries, as already noted by Elkington20 and then Pomerantz et al. in 2012,23 who described an increased risk of fracture and head injuries in association with these falls compared to falls from home furnishings.23
The main limitations of our study are that it may have missed patients that never sought care in emergency departments because the outcome of the falls seemed mild or because care was sought in primary care settings, and the lack of a subsequent followup to assess patient outcomes and detect potentially delayed effects of the falls.
In our study, we did not take into account the input of families as to the reason for the fall or whether protective–preventive measures were being used in or outside the home. We also did not use validated measures such as the Abbreviated Injury Scale (AIS) or the Injury Severity Score (ISS) to define serious injuries.
In conclusion, there seems to be a false sense of security among caregivers of children with little independent mobility, as the incidence of falls was highest in infants aged 9–12 months, especially in the home and from nursery furniture.
Based on our data, the most serious injuries occur in children aged less than 3 months for falls from heights of more than 50cm, but we did not find an association with unwitnessed falls. We also found that falls from the arms of a caregiver, stairs or that take place in the street are risk factors for serious injuries.
In light of these findings, we ought to refine or reinforce supervision measures, especially when it comes to the use of baby equipment, and emphasise preventive measures in the street, where other potential distractions can influence inattention to children.
Conflict of interestsThe authors have no conflict of interests to declare.
- 1.
Hospital General Universitario Gregorio Marañón, Madrid
- 2.
Hospital Sant Joan de Déu Barcelona, Esplugues de Llobregat
- 3.
Hospital General del Parc Sanitari Sant Joan de Déu, Sant Boi de Llobregat
- 4.
Hospital Universitario Son Espases, Palma de Mallorca
- 5.
Hospital Universitari de Girona Doctor Josep Trueta, Gerona
- 6.
Hospital Universitario Puerta del Mar, Cádiz
- 7.
Consorci Sanitari de Terrassa, Terrassa
- 8.
Hospital Universitario Infanta Leonor, Madrid
The list of the participating hospitals can be found in Appendix A.
Please cite this article as: Jiménez de Domingo A, Rubio García E, Marañon Pardillo R, Arias Constanti V, Frontado Haiek LA, Soriano Arola M, et al. Epidemiología y factores de riesgo de las lesiones por caídas en niños menores de un año. An Pediatr (Barc). 2017;86:337–343.
Previous presentation: The results of this study were presented as an oral communication at the XX Reunión Anual de la Sociedad Española de Urgencias de Pediatría, Bilbao, Spain, 2015.

Anales de Pediatría (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals