



Totally implantable venous access devices (TIVADs) or ports are used for delivery of long-term intravenous treatment, especially in children with cancer. Their insertion by surgical cut-down is being replaced by ultrasound-guided techniques, which are associated with lower rates of technique failure and complications. However, there is still debate as to which is the best access site, of which there are several options: subclavian vein, external jugular vein or internal jugular vein, among others.1 Placement of TIVADs is customarily guided by fluoroscopy, which entails exposure to ionising radiation. One possible alternative is guidance by ultrasound, although there are no data on the use of ultrasound for this purpose. We present our initial experience in the placement of TIVADs through an exclusively ultrasound-guided technique that combines ultrasound-guided puncture of the brachiocephalic vein (BCV) followed by intraoperative transthoracic echocardiography to guide catheter placement, avoiding the use of fluoroscopy.
We used this technique for 6 months to insert TIVADs. Cannulation was performed in the operating theatre by a paediatrician with experience in ultrasound-guided venous catheter insertion and a paediatric surgeon. A 12MHz linear probe was used to obtain a long-axis view of the BCV (left and right) from the supraclavicular fossa. A 21G needle was inserted at the confluence of the right subclavian vein and the BCV. The BCV was selected in every case so that the transducer could be placed on the left side of the patient, away from the surgical field. After advancing the guidewire, it was replaced by a peel-away introducer. A 6.5F catheter was inserted through the introducer in the right atrium with echocardiographic visualisation through the subcostal window with a 2–4MHz cardiac probe. Once the catheter tip could be visualised in the right atrium, it was pulled back to the cavoatrial junction. Correct placement of the catheter in the superior vena cava was confirmed in the modified parasternal long axis view (Fig. 1). At this point, the surgeon made the subcutaneous tunnel and fitted the port, after which the procedure was completed with the customary technique. Four procedures were performed in 2 boys (aged 5 and 10 years) and 2 girls (aged 11 and 15 years) with body weights ranging between 16 and 46kg. The indications for TIVAD placement were lymphoma in 3 patients and neurodegenerative disease in 1. Catheter insertion in the BCA was successful in the first puncture and the catheter was placed correctly and without associated complications in every case. The TIVADs continued to work correctly after a median followup of 9 months (interquartile range, 6–11 months).
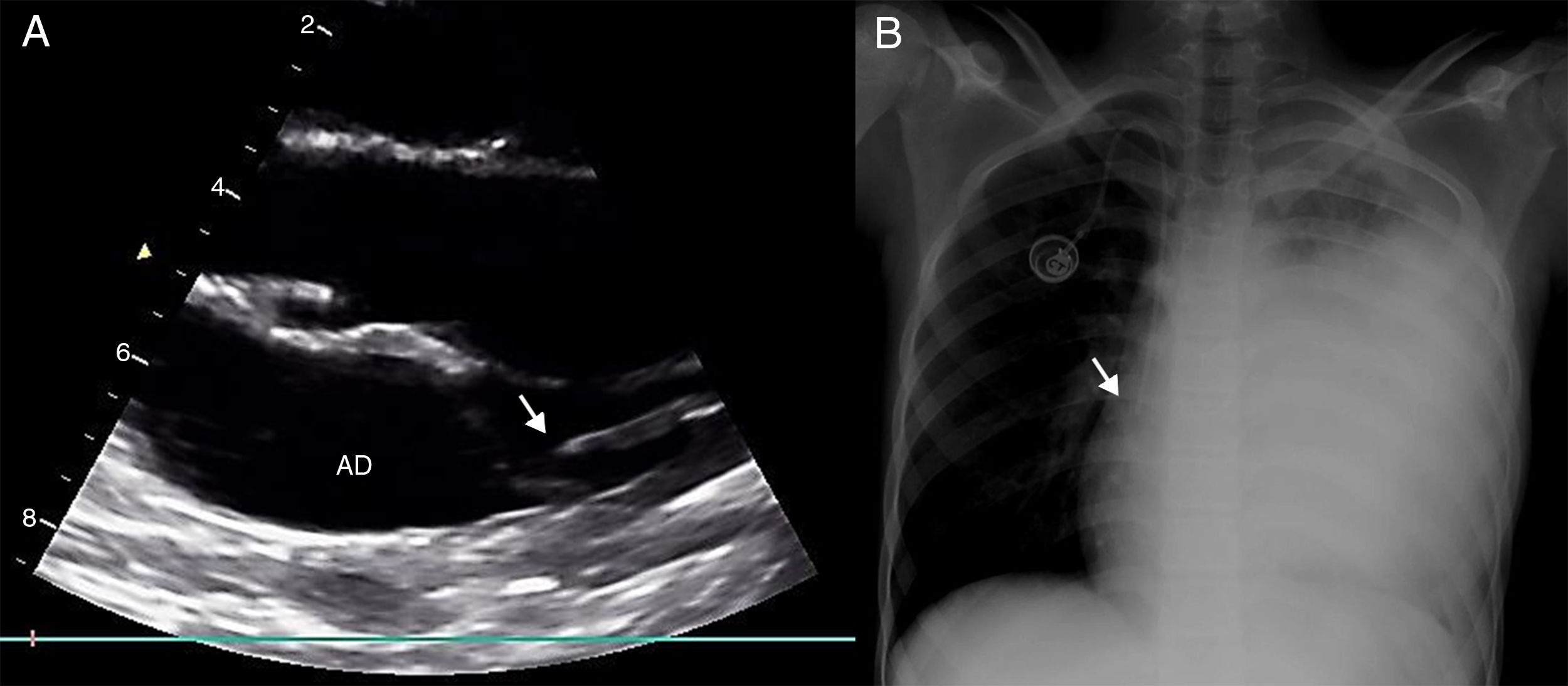
Catheter placement in the cavoatrial junction. (A) Modified parasternal long-axis view of the superior vena cava. The catheter is seen in the top of the right atrium (RA) at the cavoatrial junction. To obtain the modified parasternal view, starting from the standard parasternal view, the transducer is placed parallel to the sternum and tilted to the right side of the patient until the superior vena cava is visualised. (B) Plain X-ray of the same patient showing correct placement of the catheter.
This is the first published description of the use of an exclusively ultrasound-guided technique for placement of TIVADs. The supraclavicular in-plane cannulation of the BCV is a novel venous access that has been gaining popularity in recent years. It allows needle insertion in the longitudinal plane, with great control of its trajectory. Published studies have reported a high success rate in the first puncture attempt and a low rate of complications. Compared to the classical infraclavicular approach, needle entry in the vein is less angulated and goes in the craniocaudal direction, with a very small risk of catheter kinking or incorrect placement.2 Combined with the use of echocardiography, it allowed us to place the TIVADs without exposing the patient to radiation. Although the doses of radiation involved in the insertion of venous ports in children are usually small, in technically complex procedures the exposure can reach doses nearing those of computed tomography.3,4 Paediatric specialists in any field must strive to minimise exposure. Since children are more vulnerable to the effects of radiation, a technique that avoids fluoroscopy is of particular interest in paediatrics. Ultrasound-guided puncture not only increases the safety and efficacy of vascular access placement, but may also make it unnecessary to routinely perform an X-ray after the procedure.5 Visualisation of the superior vena cava is relatively easy and is a common task in clinical echocardiography. This is a key advantage when it comes to verification of catheter placement. Our group recently published a study that demonstrated that echocardiography was at least as effective as plain radiography in determining the location of central venous catheters in critically ill children.6 In the study presented here, we demonstrate that the use of echocardiography to guide TIVAD placement is promising, despite the patients not being ideal candidates for it, as they were relatively old children with less-advantageous echocardiographic windows. We believe that the true promise of this application resides in young children and infants, in whom catheter insertion is particularly challenging. The technique could also be used outside the operating theatre with superficial sedation and local anaesthesia as long as aseptic technique is guaranteed. This would allow insertion of TIVADs without first needing to book an operating room. To be sure, our case series is very small and our findings should be considered preliminary. As occurs in any ultrasound technique, its main limitation is the need for personnel with specific training, and TIVAD placement should not be performed without adequate previous experience (we tentatively suggest a minimum of 20 procedures to develop competence in the evaluation of catheter placement). We need to acknowledge that the use by physicians of bedside ultrasound techniques for diagnosis or procedure guidance is now a reality in the field of paediatrics.
Please cite this article as: Oulego-Erroz I, Pradillos-Serna JM, Fuentes-Carretero S, Ardela-Díaz E. Colocación de reservorios venosos centrales mediante una técnica exclusivamente ecoguiada: experiencia preliminar. An Pediatr (Barc). 2018;89:117–118.
