
Streptococcus pyogenes (S. pyogenes) is an important human pathogen that is responsible for a broad range of infections, from uncomplicated to more severe and invasive diseases with high morbidity/mortality. The M protein (emm type) is a critical virulence factor. Several studies have shown an increased incidence of invasive S. pyogenes disease. This was associated with an increase in the prevalence of M1 and M3 types, well-recognised virulent M types. The aim of the present study was to confirm the resurgence of invasive S. pyogenes disease during 2011–2018 and to identify the relationship between specific M types with disease presentation.
Material and methodsIsolates were confirmed using standard techniques: colony morphology, β-haemolysis, biochemical tests, and agglutination with specific antisera (DiaMondiaL Strep Kit, DiaMondiaL, Langenhagen, Germany). The antibiotic sensitivity was performed using microdilution (Vitek®2 Compact, bioMeriéux, Inc., Durham, NC). Molecular analysis included the determination of the emm gene and superantigen profile.
ResultsA total of 29 invasive isolates were collected (2011–2018) from blood (16), pleural fluid (9), synovial fluid (3), and cerebrospinal fluid (1). One strain per year was isolated between 2011 and 2013, with 2, 5, 4, 6, and 9 strains being isolated between 2014 and 2018, respectively. The most frequent clinical presentations were bacteraemia and pneumonia (10 and 9 cases). The predominant types were M1 (11 isolates) and M3 (3 isolates). A correlation was found between M1 and M3 types, and pneumonia (6/7 cases) and deep soft tissue infections (3/3 cases).
ConclusionsAn increased incidence of invasive S. pyogenes disease was observed during the study period, with M1 and M3 types being those most commonly isolated and associated with pneumonia and deep soft tissue infections.
Streptococcus pyogenes (S. pyogenes) es un importante patógeno humano responsable de una gran diversidad de infecciones, algunas de las cuales presentan un carácter severo con elevada morbimortalidad asociada. La proteína M es un determinante de virulencia crítico de este microorganismo. Diferentes estudios comunican un incremento de enfermedad invasora por S. pyogenes (EISP) relacionado con un aumento de serotipos M1 y M3, de reconocida virulencia. El objetivo del trabajo es confirmar el incremento observado de las enfermedades invasoras por S. pyogenes durante 2011-2018, y conocer qué serotipos pudieran estar implicados.
Material y métodosLa identificación de los aislados se realizó mediante pruebas fenotípicas convencionales: morfología de las colonias, β-hemólisis, pruebas bioquímicas y detección de antígeno A de Lancefield (DiaMondiaL Strep Kit, DiaMondiaL, Langenhagen, Alemania). La sensibilidad antibiótica se determinó mediante microdilución (Vitek®2 Compact, bioMeriéux, Inc., Durham, NC). La caracterización genotípica incluyó el gen emm y el perfil de superantígenos.
ResultadosEntre 2011-2018 se recuperaron 29 S. pyogenes invasores de sangre (16), líquido pleural (9), líquido sinovial (3) y líquido cefalorraquídeo (1). Entre 2011 y 2013, se cuantificó una cepa por año. Entre 2014 y 2018 se aislaron 2, 5, 4, 6 y 9 cepas, respectivamente. Las entidades clínicas más frecuentes fueron bacteriemia y neumonía (10 y 9 casos). Los serotipos mayoritarios fueron M1 (11) y M3 (3), asociados predominantemente a neumonía (6/7 casos) e infección profunda de partes blandas (3/3 casos).
ConclusionesSe constata un incremento de las enfermedad invasora por S. pyogenes en el periodo estudiado resultando mayoritarios, conforme a la bibliografía, los serotipos M1 y M3, los cuales se asocian con neumonía e infección profunda de partes blandas.
Genomic and molecular techniques have allowed the characterisation of a substantial number of virulence factors of Streptococcus pyogenes, or group A streptococci (GAS), knowledge that has led to the development of models of disease progression for infection by this microorganism with the aim of improving treatment and care strategies.1,2 In this context, the M protein is the immunodominant surface antigen of S. pyogenes and a critical determinant of its virulence, and the 5ʹ variable region of the emm gene that encodes this protein is analysed to type S. pyogenes strains. This region is hypervariable, resulting in a very diverse range of serotypes. Some studies have found a significant association between some of these serotypes and specific clinical manifestations,3–5 so the M protein could be considered a key marker of clinically relevant strains. In case of invasive GAS disease (IGASD), this association predominantly involves serotypes M1 and M3, which are the most prevalent worldwide.1,3,4,6–13 This association is not found in every instance,14 but nevertheless the mortality rates associated with these 2 serotypes clearly exceed those of other serotypes.
Other virulence factors, such as streptococcal pyrogenic exotoxins (SPEs), encoded by the spe gene, have also been associated with IGASD, although their activity seems to be modulated, among other factors, by the M protein,15 and therefore they may play a lesser role in the virulence of the strains that produce them. Thus, emm gene analysis in certain clinically relevant strains may be used to indirectly predict the course of the infection.
The aim of our study was to confirm the increasing trend in IGASD observed in the 2011–2018 period in the paediatric population managed in our hospital and determine the serotypes most frequently involved. The rationale for this retrospective study is the need to establish foundations for future lines of inquiry aimed not only at making a register of local IGASD cases, but also at collecting data on clinical, epidemiological and genetic variables of interest in the documentation of this disease with the ultimate goal of improving the management of affected patients.
Material and methodsWe cultured S. pyogenes isolates in Columbia blood agar (Columbia agar with 5% sheep blood; bioMeriéux SA, Marcy-l’Etoile, France) and incubated the plates at 37°C for 24h in 5% CO2. The phenotypic classification was based on colony morphology, β-haemolytic activity and Lancefield group A antigen detection (DiaMondiaL Strep Kit, DiaMondiaL, Langenhagen, Germany). The definitive microbial identification and antibiotic susceptibility testing were performed by means of biochemical and microdilution methods (Vitek®2 Compact, bioMeriéux Inc, Durham, NC, USA). We submitted the isolated strains to the Instituto de Salud Carlos III for genotyping: analysis of emm and spe genes. Analysis of the emm gene determines the M serotype of the strain. The criteria for definition of septic shock adhered to the guidelines of the consensus document of the Sociedad Española de Cuidados Intensivos Pediátricos (Spanish Society of Paediatric Intensive Care, SEPICU) and the Sociedad Española de Urgencias Pediátricas (Spanish Society of Paediatric Emergency Medicine, SEUP) on the management of severe sepsis and septic shock in the paediatric population.16
ResultsBetween 2011 and 2018, 29 strains of S. pyogenes that caused IGASD were isolated at the Hospital Infantil Niño Jesús in 29 patients aged 13 days to 12 years (median, 2 years). Tables 1 and 2 summarise the clinical presentation and molecular characterisation of the isolates. Table 1 includes serotypes M1 and M3. Table 2 presents the data for all other identified serotypes and the clinical presentation of 3 patients with nontypeable strains. We did not find differences in age or sex associated with the serotype. In the 2011–2014 period, 5 strains were isolated, of which 2 corresponded to serotypes M1 and M3 and the remaining three could not be typed. In the 2015–2018 period, 24 strains were isolated, of which 12 corresponded to serotypes M1 and M3 and the other 12 to other serotypes. Strains were isolated from blood (16), pleural fluid (9), synovial fluid (3) and cerebrospinal fluid (1). The most frequent clinical conditions were bacteraemia (10 cases) and pneumonia with pleural effusion with or without associated bacteraemia (9 cases), followed by septic arthritis (6 cases), deep soft tissue infections (3 cases) and meningitis (1 case). All patients were fully and correctly vaccinated for their age. One patient presented with pharyngotonsillitis caused by S. pyogenes concurrent with the bacteraemia. We did not identify a preceding history of wounds or surgical intervention in any of the patients. Twenty-six (90%) of the cases of IGASD were community-acquired.
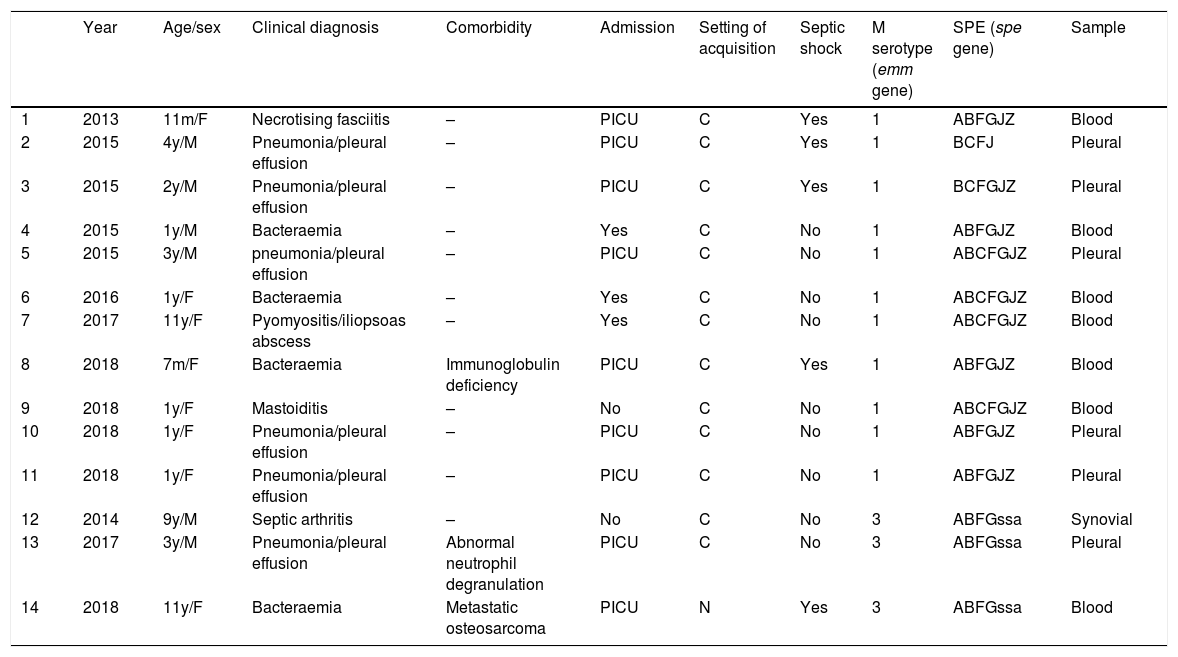
Clinical presentation and molecular characterisation of Streptococcus pyogenes strains classified as serotypes M1 and M3.
| Year | Age/sex | Clinical diagnosis | Comorbidity | Admission | Setting of acquisition | Septic shock | M serotype (emm gene) | SPE (spe gene) | Sample | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2013 | 11m/F | Necrotising fasciitis | – | PICU | C | Yes | 1 | ABFGJZ | Blood |
| 2 | 2015 | 4y/M | Pneumonia/pleural effusion | – | PICU | C | Yes | 1 | BCFJ | Pleural |
| 3 | 2015 | 2y/M | Pneumonia/pleural effusion | – | PICU | C | Yes | 1 | BCFGJZ | Pleural |
| 4 | 2015 | 1y/M | Bacteraemia | – | Yes | C | No | 1 | ABFGJZ | Blood |
| 5 | 2015 | 3y/M | pneumonia/pleural effusion | – | PICU | C | No | 1 | ABCFGJZ | Pleural |
| 6 | 2016 | 1y/F | Bacteraemia | – | Yes | C | No | 1 | ABCFGJZ | Blood |
| 7 | 2017 | 11y/F | Pyomyositis/iliopsoas abscess | – | Yes | C | No | 1 | ABCFGJZ | Blood |
| 8 | 2018 | 7m/F | Bacteraemia | Immunoglobulin deficiency | PICU | C | Yes | 1 | ABFGJZ | Blood |
| 9 | 2018 | 1y/F | Mastoiditis | – | No | C | No | 1 | ABCFGJZ | Blood |
| 10 | 2018 | 1y/F | Pneumonia/pleural effusion | – | PICU | C | No | 1 | ABFGJZ | Pleural |
| 11 | 2018 | 1y/F | Pneumonia/pleural effusion | – | PICU | C | No | 1 | ABFGJZ | Pleural |
| 12 | 2014 | 9y/M | Septic arthritis | – | No | C | No | 3 | ABFGssa | Synovial |
| 13 | 2017 | 3y/M | Pneumonia/pleural effusion | Abnormal neutrophil degranulation | PICU | C | No | 3 | ABFGssa | Pleural |
| 14 | 2018 | 11y/F | Bacteraemia | Metastatic osteosarcoma | PICU | N | Yes | 3 | ABFGssa | Blood |
C, community-acquired infection; F, female; m, month; M, male; N, nosocomial infection; PICU, paediatric intensive care unit; SPE, streptococcal pyrogenic exotoxin; y, year.
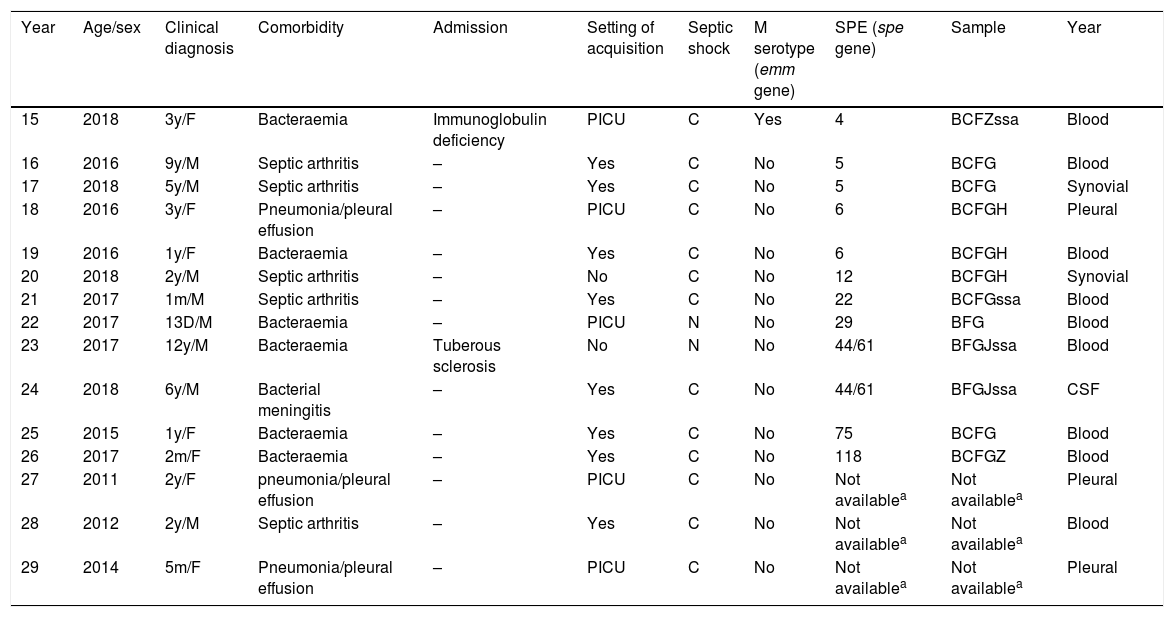
Clinical presentation and molecular characterisation of Streptococcus pyogenes strains classified as serotypes other than M1 or M3.
| Year | Age/sex | Clinical diagnosis | Comorbidity | Admission | Setting of acquisition | Septic shock | M serotype (emm gene) | SPE (spe gene) | Sample | Year |
|---|---|---|---|---|---|---|---|---|---|---|
| 15 | 2018 | 3y/F | Bacteraemia | Immunoglobulin deficiency | PICU | C | Yes | 4 | BCFZssa | Blood |
| 16 | 2016 | 9y/M | Septic arthritis | – | Yes | C | No | 5 | BCFG | Blood |
| 17 | 2018 | 5y/M | Septic arthritis | – | Yes | C | No | 5 | BCFG | Synovial |
| 18 | 2016 | 3y/F | Pneumonia/pleural effusion | – | PICU | C | No | 6 | BCFGH | Pleural |
| 19 | 2016 | 1y/F | Bacteraemia | – | Yes | C | No | 6 | BCFGH | Blood |
| 20 | 2018 | 2y/M | Septic arthritis | – | No | C | No | 12 | BCFGH | Synovial |
| 21 | 2017 | 1m/M | Septic arthritis | – | Yes | C | No | 22 | BCFGssa | Blood |
| 22 | 2017 | 13D/M | Bacteraemia | – | PICU | N | No | 29 | BFG | Blood |
| 23 | 2017 | 12y/M | Bacteraemia | Tuberous sclerosis | No | N | No | 44/61 | BFGJssa | Blood |
| 24 | 2018 | 6y/M | Bacterial meningitis | – | Yes | C | No | 44/61 | BFGJssa | CSF |
| 25 | 2015 | 1y/F | Bacteraemia | – | Yes | C | No | 75 | BCFG | Blood |
| 26 | 2017 | 2m/F | Bacteraemia | – | Yes | C | No | 118 | BCFGZ | Blood |
| 27 | 2011 | 2y/F | pneumonia/pleural effusion | – | PICU | C | No | Not availablea | Not availablea | Pleural |
| 28 | 2012 | 2y/M | Septic arthritis | – | Yes | C | No | Not availablea | Not availablea | Blood |
| 29 | 2014 | 5m/F | Pneumonia/pleural effusion | – | PICU | C | No | Not availablea | Not availablea | Pleural |
C, community-acquired infection; CSF, cerebrospinal fluid; F, female; m, month; M, male; N, nosocomial infection; PICU, paediatric intensive care unit; SPE, streptococcal pyrogenic exotoxin; y, year.
Fourteen patients (48%) were admitted to the paediatric intensive care unit (PICU) due to disease progression. Six of them met the criteria for septic shock. Two of them, who had bacteraemia and pneumonia, required extracorporeal membrane oxygenation (ECMO), and one other, who had necrotising fasciitis, required surgical debriding. Three of the patients admitted to the PICU with septic shock and bacteraemia resulting from IGASD had underlying primary or acquired immunodeficiency (osteosarcoma in 1 and immunoglobulin deficiency in 2).
In all cases of IGASD, once isolation of S. pyogenes was confirmed along with its antimicrobial susceptibility, the empirical antibiotic treatment was switched to penicillin with or without addition of clindamycin. None of the patients in the sample died. We were unable to obtain viable samples for typing in 3 cases (2 of pneumonia and 1 of septic arthritis).
The most frequent M serotype was M1 (11 strains), followed by M3 (3 strains), and these 2 serotypes combined were responsible for 54% of the cases of IGASD. The remaining strains were identified as serotypes M5, M6 and M44/61 (with 2 strains of each) and M4, M12, M22, M29, M75 and M118 (1 strain of each). Strains corresponding to the M1 and M3 serotypes were the most frequent in cases of pneumonia with pleural effusion (6 out of 7 cases) and deep soft tissue infections (3 out of 3 cases). All patients with pneumonia caused by S. pyogenes serotypes M1 or M3 required admission to the PICU, and 2 developed septic shock. Of the 3 patients with deep soft tissue infection by these serotypes, 1 (with necrotising fasciitis) was admitted to the PICU with a diagnosis of septic shock. The presentations associated least frequently with serotypes M1 and M3 were bacteraemia and septic arthritis. In the compounded group of patients with serotypes M1 or M3, 64% required admission to the PICU compared to 25% of patients with other serotypes; 36% of patients with serotypes M1 or M3 had septic shock compared to 8% of patients with other serotypes, 43% of patients with serotypes M1 or M3 had pneumonia with pleural effusion compared to 8% of patients with other serotypes, and 29% of patients with serotypes M1 or M3 had bacteraemia compared to 50% of patients with other serotypes. We found comorbidities in 21% of patients with serotype M1 or M3 compared to 17% of patients with other serotypes.
When it came to the molecular characterisation based on the expression of the spe gene, we found 12 different profiles, and all patients with the most frequent patterns (speABFGJZ, found in 5 strains, and speABCFGJZ, found in 4 strains) had infection by serotype M1. The analysis of serotype M1 and M3 strains showed that both of these profiles predominated and were associated with M1 strains, but not all strains with the M1 serotype had these gene expression profiles. A third profile that was less frequent (ABFGssa) was only present in M3 serotype strains involved in different clinical presentations: septic arthritis, pneumonia and bacteraemia.
DiscussionS. pyogenes causes a broad range of acute and chronic diseases, mainly in children and young adults, of which IGASDs, while amounting to only a small part of the total burden of disease by S. pyogenes, account for a substantial proportion of the morbidity and mortality associated with this infection.1 In 2005, the World Health Organization (WHO) estimated a global incidence of 663,000 new cases per year and a mortality of 163,000 deaths due to IGASD (with an overall case fatality rate of nearly 25%).17 Its incidence and mortality have been extensively studied in many developed countries, but not in developing countries, where the few high-quality population studies conducted to date suggest that invasive disease is more common and severe than initially estimated. In the paediatric population managed in our hospital, we found an increasing trend in the incidence of IGASD between 2011 and 2018. There was a greater than 4-fold increase in the number of cases between the first and second periods under study, from 5 cases in 2011–2014 to 24 cases in 2015–2018. Most cases of IGASD in the sample corresponded to community-acquired infections in patients without comorbidities or risk factors such as pharyngotonsillitis caused by S. pyogenes, previous surgery or traumatic injury or varicella,18,19 evincing that S. pyogenes is not necessarily an opportunistic pathogen. However, the 3 cases of IGASD in our sample that were not acquired in the community, all of them manifesting as bacteraemia, had the commonality of existing comorbidity – debilitating chronic disease (tuberose sclerosis), immunosuppressive therapy (osteosarcoma), or extreme age (neonate) – and that none occurred in the epidemiological context of a potential nosocomial outbreak. Since these patients had bacteraemia, precaution protocols were not applied, as isolation of patients with IGASD is only contemplated in case of pneumonia (droplet isolation) or cutaneous involvement (contact isolation).
To frame or study within the current body of evidence on IGASD in Spain, one of the most interesting recent studies in the literature, conducted by Suárez-Arrabal et al.,20 reported an increase in IGASD in the paediatric population, although the study did not include serotyping or analysis of virulence factors in isolated strains. In their discussion, the authors referred to this as one limitation of their study, as it precluded the identification of the potential role of specific serotypes in the severity of the IGASD cases included in the analysis. As we will discuss later on, the findings of our study may contribute, within the limitations of its retrospective design and small sample size, some information on this aspect.
Numerous studies conducted since the 1970s have documented an increase in the incidence of these infections in different geographical regions, deepened our knowledge on their molecular characteristics and analysed the potential association of virulence factors (M protein) with specific clinical features.8,10,11,21–23 Between 1970 and 1980, studies conducted in North America and the United Kingdom have documented an increase in IGASD associated with an increased prevalence of serotypes M1, M3 and M18, whose virulence is well known.15,24,25 Later studies in several European countries underscored this trend and expressed the need to establish a European network for surveillance of IGASD to remedy the fragmentary state of the available information on the burden of disease caused by S. pyogenes.26–28 A recent systematic review on the prevalence of different serotypes in IGASD in Europe and North America that included articles published between 2000 and May 2017 confirmed that M1 is the predominant serotype.3 This review included a study conducted in Spain that also reported the M1 serotype as most prevalent in the country in the 1998–2009 period and its association with a high mortality, followed in frequency by serotype M3.22 Other studies in Spain support these findings.4,22,29,30
In our sample, with data from 2015 to 2018, serotypes M1 and M3 were also most prevalent in cases of IGASD, and most frequently manifested with pneumonia and deep soft tissue infections, suggesting a degree of tissue tropism. The agreement of our results with those found in other studies was expected, but it is just as true that it was not actually known. In this regard, our findings are not novel. However, the corroboration that they provide, even within the restrictions of the aforementioned methodological limitations, allows us to establish a starting point for the development of possible prospective studies. On the other hand, our findings diverged with the high mortality of IGASD reported in previous studies. None of the patients in our series died, although some of these patients did have more severe disease with progression to septic shock, so not only was there an increase in incidence in our case series in the 2015–2018 period, but also in morbidity, with development of shock and admission to the intensive care unit, consistently with the previous literature. This more aggressive presentation of IGASD is particularly prevalent in patients with pneumonia. All of these patients required admission to the PICU due to their worsening condition, and 1 with necrotising pneumonia required repeated surgical drainage due to the persistence of empyema. Another 2 patients developed toxic shock, of who 1 required ECMO. This was not the case in patients with bacteraemia, the second most frequent clinical presentation in our series, as only a minority required admission to the PICU. When it came to cases of deep soft tissue infection, the severity of the presentation with necrotising fasciitis was not only evinced by the need for PICU admission but also for the need for surgical debridement.
In cases without predisposing factors or comorbidity, a more severe clinical presentation could be attributed at least in part to the virulence of the involved strains based on their serotype. In the multivariate analysis of a study in which serotypes M1 and M3 also predominated (21% and 11%, respectively). Vlaminckx et al.6 found that these serotypes were independently associated with streptococcal septic shock and death. In our study, the greater virulence of strains M1 and M3 was reflected in the fact that a greater number of patients with these serotypes required admission to the PICU, including some with septic shock, compared to patients with IGASD involving other serotypes. In the specific case of patients with pneumonia, our results seem to suggest the need for more aggressive management.
In addition, Vlaminckx et al.6 reported that the overall relative frequency of serotype M1 in nasopharyngeal aspirate samples was small, of only 4.5%, compared to the proportion in samples of IGASD cases, which supports the belief in the considerable invasiveness of this serotype. It would be interesting to analyse this aspect in the most prevalent M1 and M3 strains in our case series, as this could provide a hypothesis for future research projects. Nevertheless, this should not shift attention from other, less prevalent serotypes, for while they do not currently seem to be associated with specific clinical features, they could emerge in the future. Large-scale epidemiological studies have revealed variability through time in the rate of isolation of specific serotypes, with certain serotypes predominating in given periods only to be replaced by other serotypes in subsequent years.7,31 In this regard, we believe that our study, in providing current data for a Spanish case series, may be relevant by evincing the importance of the availability of local databases which, combined with national or international databases, contribute to our knowledge of the epidemiology of these serotypes as well as their surveillance and periodical control.
Besides the M protein, the severity of IGASD is determined by a host of other proteins, chiefly the SPEs.15,24,32,33 Along with the predominance of serotypes M1, M3 and M18, evidence has emerged of an association with exotoxin SpeA, found in strains that cause IGASD in North America, but not in the United Kingdom.34 This discrepancy may be due to several SPEs acting together to produce specific effects, which would make it complicated to determine their individual contribution to specific invasive disease presentations. For this reason, in our study we referred to the set of detected SPEs as spe gene expression patterns or profiles. These protein profiles would provide a more accurate representation of their behaviour as virulence factors and would facilitate the interpretation of the obtained data.
We found a broad variety of spe gene expression profiles in the strains under study, and in fact previous studies have demonstrated that there is no common SPE profile in the strains that cause IGASD.15,35 In our study, this broad range of patterns seemed to become simpler when we differentiated the patterns expressed by strains of the predominant M1 and M3 serotypes, which is why we think it appropriate to focus the discussion on this aspect on these 2 serotypes. We found an association between the 2 most frequent exotoxin profiles and the M1 serotype, but this was not in turn associated with specific clinical manifestations. A specific presentation was also not associated with the exclusive pattern exhibited by serotype M3 strains. In this regard, Metzgar et al.15 made an interesting suggestion, proposing that in addition to being a virulence factor in itself, the M protein may play a role in modulating other virulence factors such as the SPEs. This predictive power attributed to the M protein would partly explain the higher consistency we found in the comparison of specific clinical manifestations with specific M serotypes versus the exotoxin profiles expressed by the strains under study. In light of the above and our own experience in this study, the analysis of the SPE expression profile is not likely to help predict the clinical impact of different S. pyogenes strains, and the prediction of the potential invasiveness of strains should therefore focus on M protein typing.
However, while the contribution of serotyping should not be underestimated, it is not possible to establish an unequivocal association between serotype, SPE profile and clinical presentation. This is, after all, only to be expected, as the importance of the role of a specific M serotype in the proportion of IGASD should be relativised, since it probably results from the combination of the relative frequency of circulating strains of a specific serotype in a community, the invasiveness of the strain and the immunity at the individual and population levels to different strains (levels of antibodies against M protein or SPEs).8,36–38
In conclusion, our study found an increasing trend in the incidence of IGASD, with a predominance of serotypes M1 and M3 that was consistent with the literature, serotypes that seemed to be associated with pneumonia and deep soft tissue infection and, in general, severe disease. Serotyping, especially in patients with pneumonia caused by S. pyogenes, could warn of the possibility of a poor clinical outcome in patients with serotypes M1 and M3.
There are clear limitations to our study, as our results were not statistically significant due to the small sample size and the retrospective design restricted the range of variables that could be analysed. Nevertheless, we consider our study relevant in that it establishes the foundation for performance of future prospective studies with a robust statistical analysis and the participation of multidisciplinary teams that would allow the collection of high-quality data. Such studies could address aspects of interest such as the shifting trends in the prevalence distribution of serotypes involved in IGASD through the institution of reliable registers or the establishment of the rate or colonisation or non-invasive infection (pharyngitis) by S. pyogenes, as cases of IGASD could only be the tip of the iceberg when it comes to carriage of a specific invasive clade in the community.39 Along these lines, Shea et al.7 observed an increase in serotype M3 strains that caused pharyngitis that coincided with the increase in cases of invasive disease caused by the same strains. This overlap supports a disease model in which invasive strains of S. pyogenes originate from strains that cause pharyngitis and cyclical outbreaks of invasive disease coincide with or closely follow pharyngitis outbreaks. The resulting body of evidence could lead to the development of consensus documents and standardised protocols for the improved management of IGASD by health care professionals.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: González-Abad MJ, Alonso Sanz M. Infecciones invasoras por Streptococcus pyogenes (2011-2018): serotipos y presentación clínica. An Pediatr (Barc). 2020;92:351–358.
