
Obstructive sleep apnoea (OSA) is highly prevalent in children and a major public health problem. An attempt is made to determine the clinical and polysomnographic presentation of paediatric OSA in our area.
Patients and methodsRetrospective descriptive study of sleep tests conducted on children up to 14 years old from 1999 to 2012 in the Sleep Unit of the University Hospital of Albacete. Age, gender, anthropometric, clinical data, indication and variables of sleep study, treatment, and outcomes were collected.
ResultsThe study included 234 children. OSA was found in 71.8%, with 42.3% moderate and 44.6% severe. The majority were male (60.7%) and the mean age was 5 years, of whom 78% were pre-school or school age. There was overweight/obesity in 44%, with 93.4% snoring, apnoea 84.5%, and 5.4% daytime sleepiness. There were 23 polysomnographies and 145 polygraphies, with a median apnoea/hypopnoea index (AHI) of 10, SatO2 minimum 84%, desaturation index 8, and mean sleep supine 53.65% and supine events 57.61%. Treatment was lifestyle modifications 29.2%, CPAP 6%, and surgery 42.9%. Improved snoring and/or apnoea 69.4%, and weight 32.4% of overweight/obesity children.
ConclusionsMost of the studied children had a pathological AHI. Almost half were overweight/obese, and a high percentage had moderate-severe OSA. Most frequent treatment was surgery. The clinical outcome was favourable in almost 70%. Less than a third with OSA and overweight/obesity improved weight.
El síndrome de apneas-hipopneas del sueño (SAHS) es altamente prevalente en la edad pediátrica y un problema importante de salud pública. Se pretende conocer la presentación clínica y polisomnográfica del SAHS infantil en nuestro medio.
Pacientes y métodosEstudio descriptivo retrospectivo de los estudios del sueño realizados a menores de 14 años desde 1999 hasta 2012 en la Unidad del Sueño del Complejo Hospitalario Universitario de Albacete. Se recogen edad, sexo, datos antropométricos, clínicos, indicación y variables del estudio del sueño, tratamiento y evolución.
ResultadosDoscientos treinta y cuatro niños. SAHS el 71,8%: moderado 42,3% y grave 44,6%. 60,7% varones y mediana de edad 5 años; el 78% en edad preescolar o escolar. Presentaban sobrepeso/obesidad 44%, ronquidos 93,4%, apneas 84,5% y somnolencia diurna 5,4%; 23 polisomnografías y 145 poligrafías: mediana de índice de apneas-hipopneas (IAH) 10, de SatO2 mínima 84% y de índice de desaturaciones 8, y media de sueño en supino 53,65% y de eventos en supino 57,61%. El tratamiento fue medidas higiénico-dietéticas en el 29,2%, CPAP el 6% y cirugía el 42,9%. Mejoraron los ronquidos y/o apneas el 69,4% y el peso el 32,4% de los niños con sobrepeso/obesidad.
ConclusionesLa mayoría de los niños estudiados tenían un IAH patológico. Casi la mitad presentaban sobrepeso/obesidad y un alto porcentaje tenía SAHS moderado-grave. El tratamiento más indicado fue la cirugía. La evolución clínica fue favorable en casi el 70%. Menos de un tercio con SAHS y sobrepeso/obesidad mejoraron el peso.
Obstructive sleep apnoea (OSA) is characterised by repetitive episodes of cessation or significant decrease in airflow (apnoea or hypopnoea, respectively) during sleep due to anatomical or functional abnormalities in the upper airway that lead to its collapse and may be accompanied by oxygen desaturation and multiple unconscious arousals (microawakenings), all of which results in nonrestorative sleep. It may be associated with excessive daytime sleepiness (EDS) and neuropsychiatric, respiratory, endocrine/metabolic or cardiovascular diseases.1 Although one-fourth of the population experiences some episodes of apnoea or hypopnoea, OSA is only diagnosed when these episodes are very frequent and cause health problems.2
Obstructive sleep apnoea affects 4–6% of middle-aged men and 2–4% of middle-aged women,3,4 and its frequency increases with age.5 It is a public health problem of utmost importance.6 However, only 5–9% of the 1200000–2150000 individuals estimated to have the disease in Spain have received a diagnosis or been treated for it.7
Obstructive sleep apnoea can also occur in children, in whom it presents with specific manifestations. Children differ from adults on account of developmental peculiarities in the anatomy and function of the upper airway and of the neurophysiology of sleep. Paediatric OSA is a distinct entity with significant differences in aetiology, clinical presentation and treatment. The clinical manifestations and physical, cognitive and developmental outcomes of OSA in children are different compared to adults.2 Thus, the American Academy of Sleep Medicine differentiates between these two entities and includes them as separate categories in its classification of sleep disorders.8
The Consensus Document on Obstructive Sleep Apnoea in Children was published in 2011.9 It defines paediatric OSA as a disorder of breathing during sleep characterised by prolonged partial upper airway obstruction and/or intermittent complete obstruction that disrupts normal ventilation during sleep and normal sleep patterns. It presents with symptoms such as snoring, sleep disturbances and/or behavioural or learning problems.10 Severe cases may cause faltering weight, neurocognitive impairment and cor pulmonale. Several risk factors for OSA have been identified,11 the most frequent of which is adenotonsillar hypertrophy, followed by obesity, which has been emerging as an aetiological factor in children in recent years. Other factors include craniofacial anomalies, neurologic diseases such as cerebral palsy, neuromuscular disorders and gastroesophageal reflux.9
The prevalence of OSA in children is high. It affects 2–4% of children aged 2–6 years,10 and its incidence peaks between 2 and 5 years. It is most commonly found in preschool- and school-age children, but it may also manifest in the first months of life. There are no differences in prevalence between the sexes.2 Obstructive sleep apnoea is a child health priority due to its high prevalence, because it often appears in association with different chronic diseases, is associated with less favourable outcomes of these comorbidities, and has a negative impact on the quality of life of children and their caregivers.9
Our unit has been performing sleep studies in children since 1999. The number of these studies has been increasing in recent years. Patients are mainly referred due to clinical suspicion of OSA or for preoperative evaluation of patients eligible for adenotonsillectomy. The primary objective of our study was to determine the clinical and polysomnographic features of OSA in children aged less than 14 years in our region, and the secondary objective was to find the treatments used most frequently and their outcomes in terms of clinical manifestations and weight.
Patients and methodsWe conducted a retrospective descriptive study, including 234 consecutive sleep studies performed in children aged less than 14 years between October 1999 and August 2012 in the Sleep Unit of the Department of Pulmonology of the Complejo Hospitalario Universitario de Albacete.
We collected data on the following variables: sex, age, indication for sleep study, comorbidities, clinical presentation, weight, height, BMI, type of sleep study, polysomnographic/polygraphic variables, diagnosis, severity, treatment and clinical and weight outcomes.
We retrieved the data by actively searching the hospital records of each patient included in the study. The presence or absence of snoring, apnoea and EDS had been documented in every case.
We considered that the patient had comorbidities and/or adenotonsillar hypertrophy when such conditions were entered in the hospital records by a paediatrician or otorhinolaryngology specialist.
We defined obesity as a BMI at or above the 95th percentile (95P) and overweight as a BMI above the 85th percentile (85P) and below the 95P.12,13
Polysomnography (PSG) and respiratory polygraphy (RP) were always performed in our unit, and their results were analysed and interpreted by the same pulmonologist. The chief of the unit decided which type of test should be applied based on available resources and the current indications at the time of the study.
The polysomnographic/polygraphic variables included: apnoea–hypopnoea index (AHI)/respiratory disturbance index (RDI); baseline, average and lowest SatO2; percentage of total sleep time spent with SatO2<90% (T90); oxygen desaturation index of 3% or lower per hour of sleep/recording; percentage of sleep time/recording in the supine position; percentage of respiratory events in the supine position.
In its Consensus Document on OSA, the Grupo Español de Sueño (Spanish Group on Sleep) established an AHI of 1–3 as the limit of normal.2 Thus, an AHI/RDI of less than 3 was not considered abnormal. When it came to severity, OSA was classified as mild if the AHI/RDI was less than 5, moderate if it was between 5 and 10, and severe if it was greater than 10.9
Patients were treated in adherence with current indications and recommendations, in the otorhinolaryngology department if they presented with adenotonsillar hypertrophy, and otherwise in the paediatrics and/or pulmonology department.
We classified weight and clinical outcomes as improved, unchanged or worse. We categorised outcomes based on the information entered in the hospital records of patients during follow-up visits at least 6 months after initiation of treatment. Symptoms were considered to have improved if family members reported decreased snoring and frequency of apnoea, to be unchanged if they remained the same, and to be worse if they had increased in frequency or intensity, all of which were subjective assessments. Weight was considered improved if the BMI changed to a lower category (from ≥95P to 86P-94P or ≤85P, or from 86P-94P to ≤85P), unchanged if it remained in the same category, and worse if it had changed to a higher category (from ≤85P to 86P-94P and from 86P-94P to ≥95P).
The descriptive analysis consisted in the calculation of proportions for qualitative variables and of measures of central tendency and dispersion for quantitative variables. We summarised quantitative variables with the mean and standard deviation if they were normally distributed, or otherwise with the median and interquartile range (IQR).
We performed the statistical analyses and generated all charts and tables using the software SPSS version 19.0 for Windows.
ResultsA total of 234 sleep studies were performed, 148 (63.2%) in boys, and the median patient age was 5 years (IQR, 3–8.25). The reason for the study was to evaluate the need for surgery for treatment of adenotonsillar hypertrophy in 112 children (47.9%), clinical suspicion of OSA in 108 (46.2%), and other reasons in 14 (6%).
Of the 234 children under study, 168 (71.8%) had an AHI/RDI of 3 or more events per hour, which led to diagnosis of OSA. In the OSA group, 102 (60.7%) were male; the median age was 5 years (IQR, 3–8), with 82 preschool-age patients (48.8%) and 49 school-age patients (29.2%). Thus, a total of 131 patients with OSA (78%) were preschool- or school-age children.
Most of the children that received a diagnosis of OSA had no significant comorbidities. The most frequent comorbidities were diseases of the lower respiratory tract, found in 35 patients (20.8%), most commonly bronchial asthma, found in 24 patients (14.3%). However, we did not find a statistically significant association between lower respiratory disease and OSA (20.8% vs 21.2%; P=.949) or between asthma in particular and OSA (14.3% vs 15.2%; P=.866).
Of the children with OSA, 157 (93.4%) presented with snoring, 142 (84.5%) had a history of witnessed apnoeic episodes, and 9 (5.4%) had EDS. Seventy-four (44%) had excess weight, 100 (59.5%) adenotonsillar hypertrophy, and 35 (20.8%) had both.
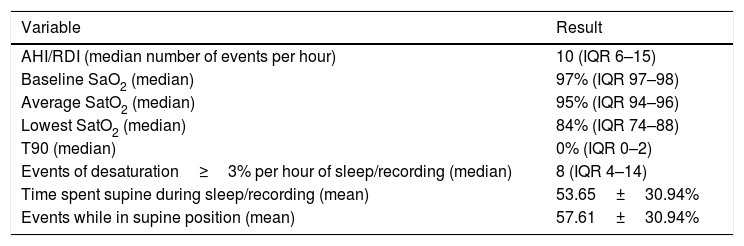
The diagnosis was made by PSG in 23 patients and by RP in 145. Table 1 summarises the relevant findings of the sleep tests.
Results of the analysis of the sleep variables under study.
| Variable | Result |
|---|---|
| AHI/RDI (median number of events per hour) | 10 (IQR 6–15) |
| Baseline SaO2 (median) | 97% (IQR 97–98) |
| Average SatO2 (median) | 95% (IQR 94–96) |
| Lowest SatO2 (median) | 84% (IQR 74–88) |
| T90 (median) | 0% (IQR 0–2) |
| Events of desaturation≥3% per hour of sleep/recording (median) | 8 (IQR 4–14) |
| Time spent supine during sleep/recording (mean) | 53.65±30.94% |
| Events while in supine position (mean) | 57.61±30.94% |
AHI, apnoea-hypopnoea index; RDI, respiratory disturbance index; IQR, interquartile range; SaO2, oxygen saturation; T90, percentage of sleep time/recording with oxygen saturation<90%.
Obstructive sleep apnoea was mild in 22 patients (13.1%), moderate in 71 (42.3%) and severe in 75 (44.6%).
In the 168 children with OSA, treatment consisted in adenotonsillectomy in 72 (42.9%), lifestyle and dietary measures (weight loss/dieting, measures to control snoring, sleep hygiene measures) in 49 (29.2%), CPAP in 10 (6%) and other treatments (such as observation and followup, topical anti-inflammatory treatment, use of a chin strap, dental devices or orthodontic intervention) in 37 (22%).
After treatment initiation, of the 157 children with a history of snoring and/or witnessed apnoeic episodes, 109 (69.4%) experienced improvement in these symptoms, 47 (29.9%) experienced no changes and 1 (0.6%) worsening of symptoms. The weight status of the 74 children with a diagnosis of OSA associated with overweight or obesity improved in 24 (32.4%) remained unchanged in 36 (48.6%) and got worse in 14 (18.9%).
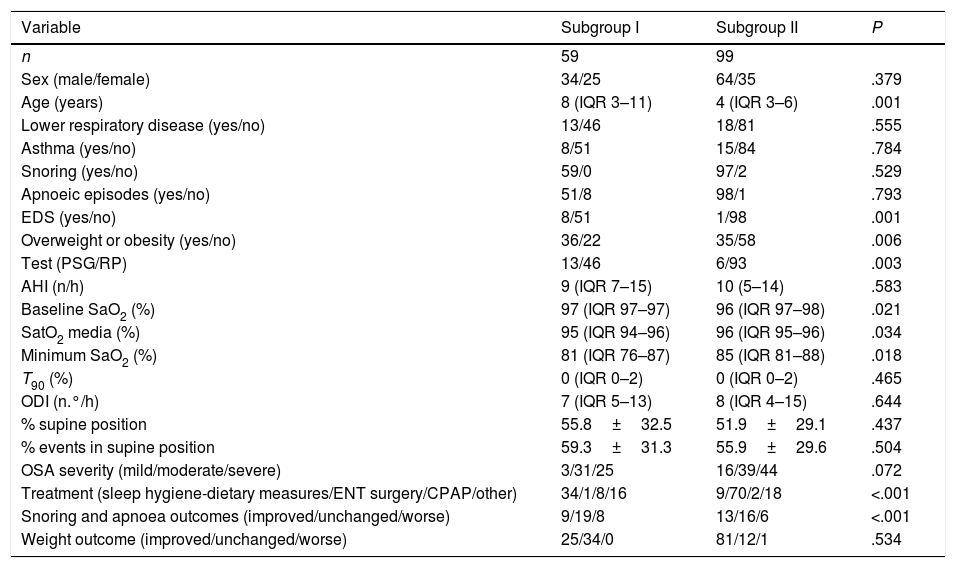
We also assessed the characteristics of 2 subsets of patients with OSA classified according to the indication for the sleep study: clinical suspicion of OSA (subset I) or evaluation of need of surgery in patients with adenotonsillar hypertrophy (subset II). Table 2 presents the results of the descriptive and comparative analysis of these two groups.
Differences between the 2 subgroups.
| Variable | Subgroup I | Subgroup II | P |
|---|---|---|---|
| n | 59 | 99 | |
| Sex (male/female) | 34/25 | 64/35 | .379 |
| Age (years) | 8 (IQR 3–11) | 4 (IQR 3–6) | .001 |
| Lower respiratory disease (yes/no) | 13/46 | 18/81 | .555 |
| Asthma (yes/no) | 8/51 | 15/84 | .784 |
| Snoring (yes/no) | 59/0 | 97/2 | .529 |
| Apnoeic episodes (yes/no) | 51/8 | 98/1 | .793 |
| EDS (yes/no) | 8/51 | 1/98 | .001 |
| Overweight or obesity (yes/no) | 36/22 | 35/58 | .006 |
| Test (PSG/RP) | 13/46 | 6/93 | .003 |
| AHI (n/h) | 9 (IQR 7–15) | 10 (5–14) | .583 |
| Baseline SaO2 (%) | 97 (IQR 97–97) | 96 (IQR 97–98) | .021 |
| SatO2 media (%) | 95 (IQR 94–96) | 96 (IQR 95–96) | .034 |
| Minimum SaO2 (%) | 81 (IQR 76–87) | 85 (IQR 81–88) | .018 |
| T90 (%) | 0 (IQR 0–2) | 0 (IQR 0–2) | .465 |
| ODI (n.°/h) | 7 (IQR 5–13) | 8 (IQR 4–15) | .644 |
| % supine position | 55.8±32.5 | 51.9±29.1 | .437 |
| % events in supine position | 59.3±31.3 | 55.9±29.6 | .504 |
| OSA severity (mild/moderate/severe) | 3/31/25 | 16/39/44 | .072 |
| Treatment (sleep hygiene-dietary measures/ENT surgery/CPAP/other) | 34/1/8/16 | 9/70/2/18 | <.001 |
| Snoring and apnoea outcomes (improved/unchanged/worse) | 9/19/8 | 13/16/6 | <.001 |
| Weight outcome (improved/unchanged/worse) | 25/34/0 | 81/12/1 | .534 |
AHI, apnoea-hypopnoea index; CPAP, continuous positive airway pressure; EDS, excessive daytime sleepiness; ENT, ear–nose–throat; IQR, interquartile range; ODI, oxygen desaturation index (SaO2≥3%); PSG, polysomnography; RP, respiratory polygraphy; SaO2, oxygen saturation; T90, percentage of sleep time with oxygen saturation<90%.
Paediatric sleep disorders are growing in importance in our region (a total of 90 children had been assessed in our unit until 2009, while the number of children assessed in 2012 was as high as 234). In recent years, OSA was clinically significant in up to 90% of children, and treatment achieved symptom control in most.
The prevalence of OSA in children is high, and the literature estimates its incidence at 2–4% of the paediatric population.10
In our area, the onset of OSA peaked between age 2 and 5 years, closely followed in frequency by school-age children. In the reviewed literature, as in our study, onset occurred most frequently in preschool- and school-age children, with no difference in prevalence between sexes.2
Adenotonsillar hypertrophy and obesity are the main risk factors for OSA in otherwise healthy children. As our study demonstrates, the most frequent cause of OSA in the paediatric population is enlargement of the tonsils and/or adenoids, and adenotonsillar hypertrophy was found in 59.5% of the patients in our sample that received an OSA diagnosis.
Obstructive sleep apnoea may also be associated with obesity, anatomical anomalies or neurologic, metabolic or muscular abnormalities.2,9 Individual susceptibility, environmental factors and lifestyle (physical and cognitive activity, diet, etc.) play an important role in phenotypic variation. Therefore, and considering the lifestyle and dietary changes that have occurred in the paediatric age group in recent years, with an increase in obesity and sedentary habits, the classic phenotype is gradually being replaced by a pattern that is more similar to the form of OSA found in adults.
In our study, 74 (44%) of the patients with OSA had overweight or obesity. This excess weight was the most likely cause of OSA in 39 (23.2%), as they did not present with adenotonsillar hypertrophy. In a study of 37 obese adolescents (BMI>97th percentile), Hannon et al. found that 45% had OSA based on the findings of PSG (OSA defined as AHI>1.5).14 Other studies have found that 47% of obese children have moderate to severe OSA, and 39% mild OSA.15,16 Redline et al. found that obesity was the strongest risk for OSA, with an OR of 4.59 (95% CI, 1.58–13.33).17 In a review of 27 studies,18 the authors found that one-third found a statistically significant association between obesity and OSA in children younger than 10 years. In fact, a literature review by Ng et al. concluded that the severity of OSA was positively correlated to the degree of obesity.19 There is variability between studies in the proportion of children with OSA reported to have obesity, which ranges between 10% and 50.6%.20–23 However, different criteria are used to define obesity, and overweight is usually not included in the analysis. A more recent study in 197 patients aged less than 18 years with sleep-associated breathing disorders found that 45.1% of them had overweight or obesity. Of these patients, 34 did not have tonsillar hypertrophy, and therefore excess weight was the main risk factor in 17.2% of the total sample.24
In our sample, 93.4% of children with OSA presented with snoring, and 84.5% had a history of apnoeic episodes witnessed by the parents. The 3 symptoms that were the strongest predictors of OSA were snoring, laboured breathing and pauses in breathing during sleep. Multiple retrospective studies have demonstrated that OSA cannot be discriminated from primary snoring based on the history and physical examination alone.25 A history of intense snoring is not sensitive enough to be an indication for surgery in children.11 Similarly, the specificity of the combination of a clinical assessment and evaluation of home video26 or audio27 recordings of a child's sleep is not high enough to confirm the diagnosis of OSA. A systematic literature review found that the positive predictive value of clinical evaluation was approximately 55% using overnight PSG as the reference test; furthermore, none of the reviewed studies found any component of the clinical evaluation to have a sensitivity and specificity greater than 65%.28 For these reasons, the American Thoracic Society11 and the American Academy of Pediatrics10 recommend PSG for assessment of paediatric OSA prior to surgery.
In our study, 5.4% of children with OSA reported EDS. The main clinical difference relative to adults is that children with sleep-associated breathing disorders usually do not experience obvious EDS and, when EDS is present, it is not predictive of OSA in young children.29
In our series, RP was the diagnostic tool used in 208 children and PSG the one used in 26. Overnight PSG is the gold standard for the detection and assessment of severity of OSA in children. However, RP could be used in the large population of children that could have OSA and thus reduce underdiagnosis, reserving PSG for children with comorbidities referred on an urgent basis for a sleep study or cases where the diagnosis is unclear or sleep disorders other than OSA are suspected.9 In uncomplicated cases, RP may correlate strongly to the findings of PSG. Several authors have noted that the combination of a clinical evaluation, a thorough examination of the upper airway, a home audio-visual recording and a RP recording performed with certified equipment offers an adequate alternative for confirmation of diagnosis in children with suspected OSA.30,31 There are few paediatric studies on the use of RP, and most have been conducted in populations at high risk of OSA, had small sample sizes and did not involve performance of PSG at the time of testing to compare the findings of both tests, leading to inconsistent results.32 A study conducted in Spain that compared both techniques concluded that RP performed in the sleep laboratory setting is a valid method for diagnosis of OSA in children.33
Resection of the tonsils and adenoids is usually the treatment of choice in children with confirmed OSA and adenotonsillar hypertrophy. In our study, adenotonsillectomy was the most frequent treatment and led to clinical improvement in 68 (94.4%) of the 72 patients treated surgically. However, this improvement was self-reported and not corroborated by performance of a new sleep study after surgery, which is a limitation in our study, as we do not know the actual number of patients that had residual OSA and therefore eligible for other interventions. Based on the current literature, adenotonsillectomy is effective in approximately 78% of cases of OSA in children,2,10,34,35 although this figure varies between sources. A Cochrane review published in 200935 remarked on the absence of double-blind studies on the treatment of paediatric OSA and concluded that the current evidence on the effectiveness of adenotonsillectomy in paediatric OSA has methodological problems, including lack of randomisation and controls and variability in the definitions and variables taken into account. A retrospective multicentre study conducted in 201022 found a cure rate of 27.2% applying a definition of cure as an AHI of less than 1 event per hour. However, the success rate rose to 78.4% if cure was defined as an AHI equal or less than 5. The authors concluded that adenotonsillectomy was associated with significant improvement in most children. However, until data from prospective multicentre studies become available, children at higher risk of residual OSA, including those aged more than 7 years, with obesity or without obesity but with asthma or severe OSA, should undergo sleep tests before and after surgery.
In our sample, CPAP was used to treat 10 patients, all of them with overweight or obesity. Patients treated with CPAP were managed at the outpatient pulmonology sleep clinic, and symptoms improved in 9 of them (90%). Continuous positive airway pressure is the second-line treatment for children with OSA,36 as most of these patients improve after undergoing adenotonsillectomy, with only a small percentage left requiring additional treatment or in who CPAP is the first-line treatment. The latter are usually children with obesity, craniofacial anomalies or neuromuscular disorders associated with adenotonsillar hypertrophy or without adenotonsillar hypertrophy.10
In addition to the limitation mentioned above, we also must remain aware of those that result from the retrospective design of the study, the predominant use of RP for diagnosis, and not having included certain symptoms that may be relevant in paediatric OSA in the analysis.
To conclude, most children that underwent a sleep study in our unit had an abnormal AHI, and a high percentage received a diagnosis of moderate or severe OSA. Nearly half of the children with OSA had overweight or obesity. The treatment prescribed most frequently was adenotonsillectomy. The clinical outcomes of treatment were favourable in nearly 70% of children with OSA, while less than one third of patients with OSA associated with excess weight succeeded in improving their weight status.
Conflict of interestThe authors have no conflicts of interest to declare
Please cite this article as: García Castillo S, Hoyos Vázquez MP, Coloma Navarro R, Cruz Ruiz J, Callejas González FJ, Godoy Mayoral R, et al. Síndrome de apneas-hipopneas durante el sueño. An Pediatr (Barc). 2018;88:266–272.
Previous presentation: This study was presented the 48 Congreso Nacional SEPAR, June 5–8, 2015; Gran Canaria, Spain.

Anales de Pediatría (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals