





Among the main social and legislative changes in Spanish family law in recent years, are (i) the increase of judicialised conflicts between parents and (ii) the enactment of the Spanish Law 26/2015, which amended the Spanish Autonomy Law 41/2002, and sought to balance the rights of minors and parents, especially minors who had not reached 16 years of age or, having reached it, faced decisions that could put their lives or health at serious risk. Likewise, recent jurisprudence has determined that, regardless of minor's age, there are sensitive “extraordinary” or “transcendent” healthcare acts, such as psychotherapeutic or surgical interventions, which require the consent of both parents, with some exceptions. All this, however, is subject to the discretion of the responsible physician, who must always ensure the best interest of the minor. Child health care therefore often raises complex conflicts involving parental rights to information and consent, especially when parental opinions differ. We present a review of the current legislative framework and the most relevant legal concepts that regulate the care of minors with regard to rights to information and minor vs. parental consent. We also present clinical guidelines for caring for minors in situations of parental conflict developed at Gregorio Marañón University Hospital in Madrid, Spain, and endorsed by the Official College of Physicians of Madrid, Spain.
Entre los principales cambios sociales y legislativos que se han producido en España en los últimos años en materia de familia, se encuentran (i) el aumento progresivo de situaciones de conflicto judicializado entre progenitores y (ii) la aparición de la Ley 26/2015 de Protección a la Infancia, que modificó la Ley 41/2002 de Autonomía del Paciente, y buscó un cierto equilibrio entre los derechos de los menores y las facultades de los progenitores, sobre todo cuando aquéllos no habían alcanzado los 16 años o la suficiente madurez o, habiéndola alcanzado, la decisión ponía en grave riesgo su vida o salud. Asimismo, se ha generado jurisprudencia que determina que, para cualquier menor de edad, existen actos asistenciales especialmente sensibles, “extraordinarios” o “trascendentes”, como las intervenciones psicoterapéuticas o las quirúrgicas, las cuales requieren, salvo excepciones, el consentimiento de ambos progenitores para llevarse a cabo. Todo ello, sin embargo, sujeto al criterio del facultativo responsable, quien debe siempre velar por el mejor interés del menor. La asistencia a menores plantea, por ello, en ocasiones, conflictos complejos en materia de información y consentimiento por parte de los progenitores, sobre todo cuando la opinión de estos no es coincidente. Presentamos una revisión del marco legislativo vigente y de los principales conceptos jurídicos que regulan la asistencia a menores en materia de información y consentimiento relativos a la salud, así como un protocolo asistencial para la atención a menores en situaciones de conflicto entre progenitores, desarrollado en el Hospital Gregorio Marañón de Madrid y avalado por el Ilustre Colegio Oficial de Médicos de Madrid.
The provision of health care to minors gives rise to complex dilemmas concerning the ability of the minor to make decisions and the rights and duties of parents in decision-making. It is an area on which multiple ethical and legal principles converge, sometimes in evident contradiction to one another, and some can be interpreted in different ways. The very legal principle of the “best interests of the child”, which is the foundation of all decision-making in health care, can have a double meaning, either attributing autonomy and the ability to make decisions to the minor, when the latter is mature enough to understand and assume the consequences of medical treatment, or excluding the minor from decision-making to act in the minor’s best interests (for instance, when the minor, despite being mature enough, makes a decision regarding a major intervention or one that poses a serious risk to the minor’s life or integrity, for example, in rejecting or refusing treatment).1,2
The provision of health care to minors gives rise to complex dilemmas concerning the ability of the minor to make decisions and the rights and duties of parents in decision-making. It is an area on which multiple ethical and legal principles converge, sometimes in evident contradiction to one another, and some can be interpreted in different ways. The very legal principle of the “best interests of the child”, which is the foundation of all decision-making in health care, can have a double meaning, either attributing autonomy and the ability to make decisions to the minor, when the latter is mature enough to understand and assume the consequences of medical treatment, or excluding the minor from decision-making to act in the minor’s best interests (for instance, when the minor, despite being mature enough, makes a decision regarding a major intervention or one that poses a serious risk to the minor’s life or integrity, for example, in rejecting or refusing treatment).1,2
The enactment of Law 26/2015 of July 8, modifying the child and adolescent protection system established in Law 41/2002 of November 14, the basic law on the autonomy of the patient and the rights and duties pertaining to health care information and records, unified the regulation of the rights of minors with unambiguous criteria that were lacking in health care legislation and attempted to resolve the problems that arose in the interpretation of the provisions for consent by proxy of minors, thus balancing the rights of parents to be informed and to consent by proxy and the right of minors to their integrity, autonomy and privacy. In addition, this law dictated that health care decisions had to be made always seeking the best interests of the child in life and health. Obviously, the “best interests” concept creates complex problems, as minors, parents, clinicians and governmental authorities may disagree in its interpretation.3 This principle can also result, depending on the specific case, in granting increased autonomy to the minor or, on the contrary, providing increased protection to the minor and therefore limiting autonomy.
The complexity of these issues is further complicated by the increase in recent years in the frequency of custody disputes between parents in Spain. In these situations, disagreements between parents, minors and clinicians in charge of patients are common, resulting in significant clinical, ethical and legal dilemmas in health care delivery, such as one of the parents refusing to consent to a treatment for a minor.4
The aim of this article is two-fold: (i) to provide a summary of current legislation and the legal concepts that regulate health care delivery to minors as concerns health-care related information and consent, and (ii) to provide a protocol with recommendations for the management of information and consent in health care delivery in situations of parental conflict. The objective is to promote knowledge and prevention of conditions that foster conflict and, should conflicts emerge, to prevent interference with the care of the minor, the potential weaponization of minors and health care providers and possibly the emergence of abusive situations.
Part I: current legal framework in Spain (2020)Given the complexity of the current legal framework, our intent is not to provide a detailed explanation of it. However, there are several rules and concepts that, in our opinion, any health care provider working with minors should be aware of, which we summarise in a series of points and present in Table 1.
Legal framework and concepts regarding the provision of health care services to minors.
| 1.1. Legal principles |
| Principle of the best interests of the child: health care interventions and parental decisions must always pursue the best interests of the minor and respect the dignity of the minor |
| Principle of good faith: legal presumption that the “care-seeking” parent acting without the other parent (the “absent” parent, in case of joint legal custody) is doing it in pursuit of the best interests of the minor, having informed and obtained consent from the other parent (which is the duty of the care-seeking parent). Still, the provider must take basic steps to verify this at first contact |
| 1.2. Spanish Civil Code |
| Legal custody: rights and duties of the parents in relation to their non-emancipated minor children up to age 18 years. Legal custody is not based on living with the minor. It involves rights and duties as regards information and consent by proxy in the context of health care delivery |
| Physical custody: daily care and assistance provided to minors. This role is defined by the situation of living with the minor |
| Parental separation: the most frequent situation is joint legal custody with physical custody assigned to one or both parents by mutual agreement or by court ruling. Sole legal custody is very rare |
| 1.3. Law 26/2015 on the Protection of Children and Adolescents modifying Law 41/2002 on Patient Autonomy |
| Informing parents and consent by proxy: cut-off age, 16 years* |
| <16 years: parents decide in every case |
| ≥16 years: the minor decides in every case, except for: |
| Ordinary interventions in minors with diminished decision-making capacity (physical/mental condition) |
| Interventions posing a serious risk to the health of the minor |
| Major/extraordinary interventions |
| Clinical trials, voluntary termination of pregnancy, assisted reproductive technology |
| * Law 41/2002 stipulated that “mature minors” aged 12–16 years did not require consent by proxy and that even in case of high risk, parents had to be informed and their opinion taken into account, but the decision always rested with the minor. Law 26/2015 establishes that when it comes to minors aged less than 16 years, any health care intervention (even in the care of what Law 41/2002 referred to as a “mature minor”) requires obtention of consent by proxy from the parents, all the while considering the opinion of the minor and whether the maturity of the minor justifies taking this opinion into account |
| 1.4. Jurisprudence (court rulings) |
| 1.4.a) Ordinary versus extraordinary care |
| Always based on the judgment of the clinician* |
| Minor intervention/ordinary care: mild accidental injuries, mild diseases, paediatric checkups, vaccines recommended by health care authorities |
| Major/extraordinary intervention: aggressive preventive, palliative or curative treatments, medico-surgical interventions, mental health or psychiatric treatment |
| 1.4.b) Information and consent by proxy: one or both parents? |
| Urgently needed intervention: a single parent suffices |
| Banal/ordinary interventions: <16 years = a single parent suffices/≥16 years: the minor decides |
| Major/extraordinary interventions: always both parents (in case of joint legal custody) |
| *The more significant or irreversible the consequences of the decision to be made are, the more important it is that the provider correctly assess the maturity of the minor and the risks to the minor involved in the current situation and the decision to intervene versus not intervene |
| 1.5. Art. 156 of the CC and RDL 9/2018 |
| Exceptions in which a single parent suffices in circumstances that would usually require both parents |
| RDL 9/2018: Court sentence or ongoing trial of one of the parents for violating the liberty, moral integrity or sexual liberty and health of a minor or underage child of both parents |
| Art. 156 CC: Court ruling conferring parental authority to one of the parents when there is disagreement between them |
| Art. 156 CC: In the absence thereof, or as a result of the absence, incapacity or impossibility of one of the parents |
1.1) Legal principles of the “best interests of the child” and “good faith”, which constitute the foundation of the current legal framework and health care protocols.
1.2) Concepts of legal and physical custody (defined by the Spanish Civil Code) and their implications in health care information and consent by proxy for underage patients.
1.3) Regulatory changes introduced in Law 26/2015, modifying Law 41/2002, to balance the rights of parents to be informed and consent by proxy and the right of minors to their integrity, autonomy and privacy. This law established the age of majority of the individual as regards health care at 16 years, with exceptions detailed below, and introduced modifications in the types of health care services that would require informing the parents and obtain consent by proxy based on this age threshold and the definition of “minor/ordinary” care versus “major/extraordinary” interventions.
1.4) Qualifications introduced by legal practice (court rulings)
1.4.a) Definition of major/extraordinary intervention versus minor intervention/ordinary care. The amendment to Law 41/2002 introduced by Law 26/2015 established a legal difference between services or interventions that may (or will not) pose a serious threat to the life or health of the minor, with an emphasis on the capacity of minors aged 16 or more years, although it does not provide a detailed list of the services of interventions included in these categories. In any case, Law 41/2002 explicitly establishes that this distinction will be made taking into account the clinical judgment of the provider in charge of the patient (“based on the judgment of the clinician”). Thus, if the clinician considers the intervention “major” or “extraordinary”, the autonomy of the minor aged 16 or more years is restricted and the decision of the parents will have to be based on what is best for the life or health of the minor they represent by proxy (principle of beneficence), and in no case can be a decision with harmful consequences. Based on the principle that the judgment of the clinician must be taken into account and the fact that Law 26/2015 does not define the distinction in detail, the legal system has been determining the ordinary or extraordinary nature of specific health care services or interventions over time.
1.4.b) Types of services/interventions requiring informing and obtaining consent from one versus both parents. When it comes to “urgent intervention”, the Civil Code (CC) clearly establishes that the actions taken by only one parent in situations requiring urgent care are valid. However, current laws do not clearly establish the distinction between “ordinary” versus “extraordinary” types of care. As a result, court rulings have been gradually establishing in detail who is responsible for giving consent in each type of service or intervention.
1.5) The exceptions in which it would suffice to inform or obtain consent from only one of the parents (in cases that would in theory require consent from both), independently of the age of the minor and the type of service/intervention, established in article 156 of the CC and its amendment, introduced 2018 by Royal Decree of Law 9/2018, of 3 August, on urgent measures for the implementation of the National Pact against Gender-based Violence (RDL 9/2018).
Fig. 1 presents a flow chart that summarises recommendations for the health care field based on the age of the minor and the type of action according to current law.
Part II: protocol for the management of information and consent by proxy in situations of parental conflict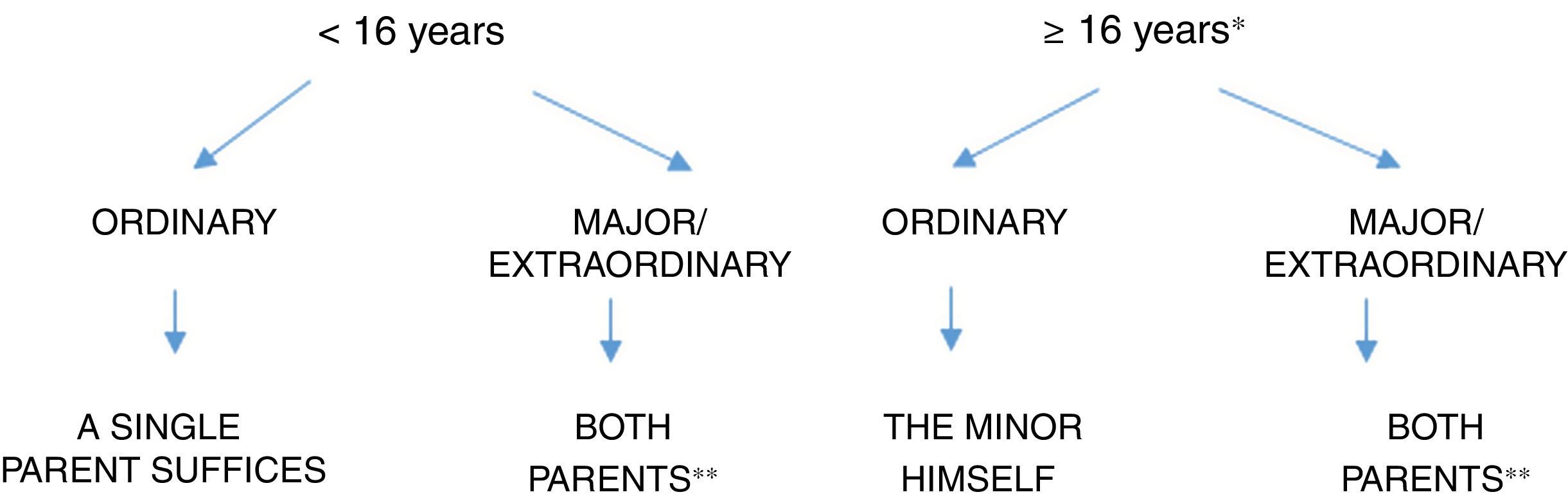
Having clarified, based on current law, which situations or health care interventions require informing and obtaining consent from the parties that have legal custody of the minor, and, more specifically, when both parents need to be involved (Fig. 1), we devote the following section to the protocol established in the Hospital General Universitario Gregorio Marañón of Madrid to address the different levels of parental conflict that can be met in health care practice and the corresponding recommendations applicable to each. This protocol was developed by psychologists and psychiatrists that care for minors with input from other professionals, including paediatricians, paediatric surgeons, social workers and legal professionals, and has been endorsed by the Official Board of Physicians of Madrid. It applies to any form of care delivered by clinicians in the health care setting, including evaluation (physical, psychological, performance of invasive diagnostic tests) and treatment (pharmacotherapy, surgery or psychotherapy, among others). A summary of this protocol can be found in Table 2.
Protocol for the management of health care information and consent by proxy in the care of minor children in case of known or suspected parental conflicta.
| A. Issues that emerge in care delivery to a minor accompanied by only one parent |
| Level I. Good faith |
| It is presumed that the care-seeking parent has informed the absent parent, as obligated in the exercise of joint legal custody |
| Nevertheless, it is always important to explore/ask basic questions about these circumstances documenting it in the health record, and not to base care delivery in mere presumptions that have not been minimally discussed with the care-seeking parent |
| The provider can evaluate the minor and determine whether the presence of the absent parent is required to complete the assessment |
| Levels II, III, IV. Good faith cannot be presumed or is in question |
| Consult with social work department |
| II. One parent has sole legal custody |
| Good faith is presumed, the minor evaluated, and treatment initiated if necessary |
| The SW subsequently confirms sole legal custody, files the corresponding documentation and activates an alert in the EHR |
| III. The provider is aware of conflict between the parents |
| The minor will be evaluated if the clinician considers it to be in the best interest of the child. The clinician decides whether an appointment must be made with the other parent (notifying parent of the appointment by official postal service fax or certified mail). |
| Consent from both parents is required to perform an intervention/treatment. The first attempt should be made by the care-seeking parent (who is legally obligated to do so). If this is not possible or entails a risk, the clinician (with or without the SW or administration) attempts to obtain consent. If no response is obtained within 30 days, tacit consent is assumed in consideration to the best interests of the child. The attempts to contact the parent will be documented |
| The SW files the corresponding documentation and activates an alert in the EHR |
| IV. The clinician is aware of the explicit objection of one parent to the intervention or there is risk involved in informing the parent |
| The minor is evaluated if the clinician considers this in the best interest of the minor |
| Support from legal authorities is sought to proceed with intervention/treatment (court or prosecutor’s office) |
| SW files the relevant documentation and sets the alert in the EHR |
| B. Conflicts involving informing the absent parent |
| Parents have the duty to keep one another informed (good faith) and the clinician is under no legal obligation to inform both parents |
| If they so request, both parents have a right to receive information separately (for example, a report with the information deemed relevant by the clinician with the possible omission of sensitive information provided by third parties and subjective notes) |
| Health records are only provided through the institution managing the case (excluding subjective notes and sensitive information provided by third parties) |
EHR, electronic health record; SW, social worker.
Applicable to any form of health care that requires informing/obtaining consent from both parents whether the minor is aged more or less than 16 years (Fig. 1).
Level I (good faith). This is what is expected in most situations. For the purposes of the initial evaluation, the presumption will be made, conforming to the principle of good faith, that the care-seeking parent has informed/will inform the absent parent about the consultation, as well as the results of the consultation and their implications, and that the care-seeking parent will fulfil the parental duty to inform the other parent and seek their consent to initiate any form of care. However, the provider must make a basic exploration of this issue in the initial interview and document this appropriately in the health record. In any case, under this presumption the provider can proceed with the evaluation of the minor and performance of non-invasive diagnostic tests in the course of as many visits as the provider deems necessary, as this is the right of the minor. The provider will determine the need to schedule an appointment with the absent parent to share the results of the evaluation or obtain further information if it is deemed pertinent in the evaluation process as dictated by the best interests of the minor (although we must reiterate that the provider is not obligated to do so). The request to set this appointment may be made by telephone, certified mail or official postal service fax.
Levels II, III and IV. In all these levels, absence of good faith is presumed or at least there are concerns about good faith. In every case, consultation with a social worker is recommended, who will receive all relevant documentation of the “conflict” (any contact with the courts, written consent forms, etc), verify it and include it in the health record of the minor along with any additional documentation of notes deemed necessary. In any of these levels, if the health information system in use allows the activation of alerts in electronic health records, it can be very useful for the social worker to request that the administrative department activate a specific alert warning any provider of the specific conflict at hand allowing the clinician and the social worker responsible for the care of the patient to edit the alert dynamically.
Level II. The care-seeking parent that accompanies the minor reports having sole legal custody of the child. The provider, while holding the presumption that the care-seeking parent is stating this in good faith and proceeding with caring for the patient, will ask the parent to provide proof of the custody order to the social worker, who in turn will confirm the sole custody of the child, file any relevant documentation and, if possible, request activation of the alert in the health record of the minor as described above.
Level III. The care-seeking parent clearly expresses from the outset (or hints or concerns emerge during the initial interview) that there are problems in communicating or disagreements about consent between the two parents. In such cases, it is of paramount importance to distinguish between the type of care being provided: evaluation or intervention, as the way to proceed differs based on it. The evaluation of the minor can always be initiated and completed with the consent of only the care-seeking parent if the clinician in charge considers it necessary based on the best interests of the child (as this is a right of the minor), mainly to assess the potential serious our urgent need for further evaluation or intervention expressed by the care-seeking parent. Notwithstanding, the clinician should remind the care-seeking parent of the duty to inform the absent parent of the visit made for evaluation and its results. If the care-seeking parent exhibits any resistance or reluctance to do so, the clinician may, as is the case in Level I, schedule a separate appointment with the absent parent to complete the evaluation following the same steps. On the other hand, intervention always requires informing and obtaining consent from both parents (with the exceptions detailed in Fig. 1). In these cases, providers will remind the care-seeking parent that it is him/her that needs to attempt to obtain the consent from the absent parent, either by informing the absent parent of a subsequent appointment (which can be attended by both parents or the absent parent only) or by obtaining written consent from the absent parent. If the relationship between the parents is fairly cordial despite the conflict, the absent parent will be invited to come to the next appointment, when the collection of information will be completed, and informed consent obtained (preferably in writing). Otherwise, providers may suggest that parents communicate through their lawyers. If communication between the parents is not an option, the clinician will attempt to contact the absent parent. The offer of an appointment will be sent by official postal service fax or certified mail through the administrative department of the health care institution employing the clinician. It is recommended that the appointment be scheduled 30 days following the date that the minor received care, as this is the number of days that the postal service allocates for the receipt of an official fax and to confirm delivery to the sender, as requested, which implies receipt of the appointment scheduling notice. The tracking number will be provided to the social worker to be entered in the health record, thus ensuring traceability of the notice. Once the administrative department receives confirmation of the delivery, it will inform the clinician and social worker. The appointment scheduling notice and the confirmation of receipt will be given to the social worker for filing. Once the absent parent has been properly informed of the situation of the minor, if the absent parent fails to show to the appointment scheduled 30 days after or to contact the provider to reschedule the appointment or clearly express (with pertinent documentation of the fact) disagreement with the performance of the intervention in the minor, it is fair to assume that the absent parent does not object to the intervention and proceed with it, interpreting the lack of response as tacit agreement. The actions taken to contact the absent parent should be documented in detail in the health record, along with the date of the scheduled appointment that the parent did not attend and the lack of properly documented communications on the part of this parent.
If the provider is informed that the absent parent cannot be contacted or his/her whereabouts are unknown, obtaining authorization from the court is recommended or, failing that, documenting in detail in the health record (in case of intervention) the ongoing situation, any attempts made to locate the absent parent and their failure, as well as obtaining a signed written statement by the care-seeking parent (to be added to all other relevant documents) declaring ignorance of the current whereabouts of the absent parent and the commitment to provide accurate contact information for the absent parent as soon as it becomes available. In any case, any reluctance or barriers exhibited by the care-seeking parent that hinder the obtention of informed consent by the absent parent should raise a red flag for providers, as this would increase the risk of malpractice in relation to the minor. For instance, if the care-seeking parent refused to give the provider the necessary information to schedule the other parent (bringing up arguments or excuses of any kind), the intervention should be deferred until appropriate consent is obtained from the absent parent or, in case such attempts fail, the court gives authorization.
Level IV. In cases in which the care-seeking parent and the absent parent do not reach an agreement by the end of Level III, or the absent parent explicitly opposes delivery of care, or cases in which informing/seeking consent of the absent parent could put the minor or a third party at risk (for instance, cases in which there have been previous reports or suspicions of abuse), the clinician must differentiate between evaluation and intervention. Evaluation is held to the same criteria applied in Level III, that is, can be initiated and completed with the consent of a single parent if the clinician in charge considers it necessary. However, as is the case in Level III, intervention would require consent from both parents, and therefore the provider must attempt to inform the disagreeing parent, if possible, of the clinical reasoning supporting the intervention and obtain consent. If consent is not obtained, cannot be obtained or seeking it poses a risk to the safety of the minor or the family, the care-seeking party or the provider could seek support from the law and wait until the competent legal authority decides whether care should be initiated, continued or interrupted. The judge can authorise the provision of care without the consent of the disagreeing parent. However, if the delay in initiating an intervention or the interruption of an ongoing treatment can pose a risk to the physical or mental health of the minor, the intervention can be initiated or maintained while awaiting the decision of the legal authorities.
Emergencies or high-risk situations: applicable to any level of careIn case of urgent need (for instance, hospital admission) evaluation and treatment may be initiated with the consent of a single parent. Right after, the clinician in charge will notify the competent court directly or through the prosecutor’s office by means of an urgent fax and will continue caring for the patient until the court decides whether care should proceed or be discontinued.
B. Conflicts regarding informing the absent parentConforming to the good faith principle and the duty of parents to communicate with each other, it does not fall to the clinician to systematically inform both parents or to do duplicate reports or letters unless they are requested to do so. Although it is a right of the parent (to be informed, request reports or obtain a copy of the health records of the child), the parent would have to expressly request it. If a parent requests a copy of the health records, health professionals in the public health system will inform the parent of the appropriate channels to pursue this request. They will in no case directly provide a copy of the health records, but instead refer the parent to the system/institution responsible for the management of health records. In every case, it is possible to withhold subjective notes entered by health care professionals and sensitive information provided by third parties. Some health information systems offer the option of including “confidential notes” in health records, which can be very useful.
ConclusionsThe key legal aspects that any clinician working with minors needs to know are the following: 1) Law 26/2015 on the protection of minors, currently in force, places some limits on the rights of minors and attempts to find a balance between their rights and the powers of parents in exercising legal custody of the child, especially when minors have not reached a certain age or level of maturity or in cases in which this age or maturity has been reached but the decisions being made pose a significant risk to the life or health of the minor; 2) Notwithstanding, when it comes to making health care-related decisions, the law still gives precedence to the judgment of the clinician, as clinicians are the individuals responsible for preserving the life and health of the paediatric population,; 3) it is the responsibility of parents that share custody of the child to exchange information about any initiated or completed health care processes in accordance with the principle of good faith. Only when the conflict is apparent and it is clear that the information will not be conveyed should the clinician actively seek the consent of the other parent, unless it poses a risk to the minor and the family; and 4) it is very important to document every decision made during care delivery to the minor and any interaction/lack thereof with the parents along with the corresponding rationale.
FundingThe study received the support from the Ministry of Science, Innovation and Universities, Instituto de Salud Carlos III, CIBERSAM, Community of Madrid (R&D grants in Biomedicine B2017/BMD-3740 AGES-CM-2), European structural and investment funds, Seventh Framework Programme, European Regional Development Fund, A Way to Make Europe; Horizon H2020 (PRISM [115916] and AIMS-2-TRIALS [77394] projects), Network of European Funding for Neuroscience Research (ERA-NET NEURON); Fundación Familia Alonso, Fundación Alicia Koplowitz and Fundación Mutua Madrileña. LPC has received funding from the Ministry of Science, Innovation and Universities, Instituto de Salud Carlos III and Fundación Alicia Koplowitz.
Conflicts of interestThe authors have no conflicts of interest to declare.
Members of the CONFLPADRES protocol working group: Dr Carmen Miranda, Dr Constancio Medrano, Dr Jesús López-Herce, Dr Manuel Sánchez Luna, Dr María Dolores Madrid Blanco, Dr Teresa Távora, Dr María Pilar Alonso, Dr María del Carmen Oria, Dr María José Toribio Vicente, Dr María Aránzazu López Rubio.
Appendix Alists the members of the CONFLPADRES protocol working group.
Please cite this article as: Pina-Camacho L, Vidal J, Picouto MD, Ortiz EJ, Jääskeläinen FM, Moreno C, et al. Atención a menores con progenitores en conflicto en materia de información y consentimiento relativos a la salud de los hijos. Protocolo asistencial en el contexto de la legislación vigente. An Pediatr (Barc). 2021;94:338.

Anales de Pediatría (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals