
Pyogenic sacroiliitis (PSI) is a rare condition that accounts for 1–2% of all joint infections in the paediatric age group. Its diagnosis is often difficult and delayed due to its nonspecific signs, symptoms and physical findings. Also, the identification of the causative microorganism is frequently challenging due to a high rate of negative blood cultures and the risks involved in joint aspiration in this location.
Patients and methodsWe performed a retrospective review of the health records of all patients aged less than 18 years admitted to a tertiary children's hospital due to PSI between 2008 and 2016.
ResultsSix cases of paediatric PSI were identified. The blood cultures were negative, and identification of the causative agent required joint fluid aspiration in one case of Aggregatibacter aphrophilus infection and specific screening tests for other less frequent agents: Kingella kingae (n=2), Brucella melitensis (n=1) and Bartonella henselae (n=1). The patients were treated with specific antimicrobial regimens, and all had favourable clinical outcomes and were free from sequelae during the follow-up.
ConclusionsDespite the small sample size, our study emphasizes the low effectiveness of blood cultures for diagnosis of paediatric PSI. It also highlights the need for a high level of suspicion for atypical agents and the early use of adequate diagnostic methods, including imaging and serological testing or polymerase chain-reaction (PCR) analysis of blood samples, as well as the prescription of an effective antimicrobial therapy.
La sacroileítis piógena (SIP) es una entidad infrecuente que representa del 1 al 2% del total de las infecciones articulares en la edad pediátrica. Su diagnóstico a menudo se complica y retrasa debido a la inespecificidad de sus síntomas, signos y exploración física. Además, la identificación microbiológica puede resultar difícil debido a la alta proporción de hemocultivos negativos y los riesgos implicados en la aspiración de líquido articular en esta localización.
Pacientes y métodosRevisión retrospectiva de las historias clínicas de todos los pacientes menores de 18 años ingresados en un hospital infantil terciario con SIP en el período 2008-2016.
ResultadosSe identificaron 6 casos de SIP en niños. Los hemocultivos fueron negativos, y la identificación del agente etiológico requirió aspiración de líquido sinovial en un paciente con infección por Aggregatibacter aphrophilus y pruebas específicas para la detección de agentes menos frecuentes en los pacientes restantes: Kingella kingae (n=2), Brucella melitensis (n=1) y Bartonella henselae (n=1). Los pacientes recibieron regímenes de antibioterapia específica, y todos presentaron una evolución favorable y libre de secuelas durante el seguimiento.
ConclusionesA pesar del reducido tamaño muestral, nuestro estudio puso de relieve la baja efectividad del hemocultivo en el diagnóstico de la SIP pediátrica. También evidenció la necesidad de mantener un elevado índice de sospecha de los agentes atípicos y de emplear precozmente métodos diagnósticos apropiados, como las pruebas de imagen y la reacción en cadena de la polimerasa (PCR) en muestras de sangre, así como la prescripción de antibioterapia efectiva.
Pyogenic sacroiliitis (PSI) is a rare condition that accounts for 1–2% of all joint infections in the paediatric age group.1–4 Its diagnosis may be difficult due to its nonspecific signs, symptoms and physical findings, often resembling other causes of back pain. At the time of admission, the disease is initially not suspected in 50% of patients,5 and this delay in diagnosis can result in increased morbidity and long-term disability. Pyogenic sacroiliitis commonly presents with fever and a limp with poorly localised pain and normal range of motion of the hip.5,6 The most sensitive clinical sign is the FABER test: pain is caused or exacerbated at the sacroiliac joint when positioning the contralateral hip in flexion (F), abduction (AB), and external rotation (ER).7 Magnetic resonance imaging (MRI) has improved sensitivity in the diagnosis of PSI and is now considered the gold standard for the early diagnosis of sacroiliitis and osteoarticular infections in general.5,6 The laboratory findings are unspecific, and positive blood cultures, osteoarticular fluid aspiration or biopsy are still considered essential for identifying the causative microorganisms.8 Historically, Staphylococcus aureus has been the most frequently identified aetiological agent .3,5 However, there has been increasing evidence that Kingella kingae is an important cause of PSI in children aged 6 months to 4 years.6,9 Identification of the causative agent is important, as an appropriate antibiotic regimen usually provides rapid resolution of symptoms and healing without the need to resort to invasive procedures.
Our aim was to characterise the epidemiological, diagnostic and clinical profile of patients with PSI admitted to our tertiary care children's hospital.
Patients and methodsWe performed a retrospective review of the hospital health records of all patients aged less than 18 years admitted to our tertiary care children's hospital in Lisbon, Portugal, with a diagnosis of PSI (ICD-9 720.2) between 2008 and 2016. We also analysed demographic and predisposing factors, clinical signs and symptoms, laboratory and imaging test results, type and duration of treatment, clinical outcome and sequelae.
ResultsSix patients were identified. The distribution by sex was homogeneous, and the mean age was 6.3 years (range, 13 months–14 years). Three were toddlers aged 12–27 months, and three were older than 7 years (range, 7–14 years). All had been healthy before the episode, and half reported recent manifestations of an acute upper respiratory infection. All patients presented with fever, limping and pain at different locations (lower limb, lumbar region and ipsilateral iliac fossa) (Table 1). Clinical documentation for the FABER test was available in 4 patients, all of whom had positive results. At admission, the mean leucocyte count was 14,933μL−1 (range, 9500–22,500), the mean C-reactive protein level was 99mg/L (range, 33–139mg/L), and the mean erythrocyte sedimentation rate (ESR) 39mm/h (range, 2–92mm/h). The results of blood cultures were negative in all patients.
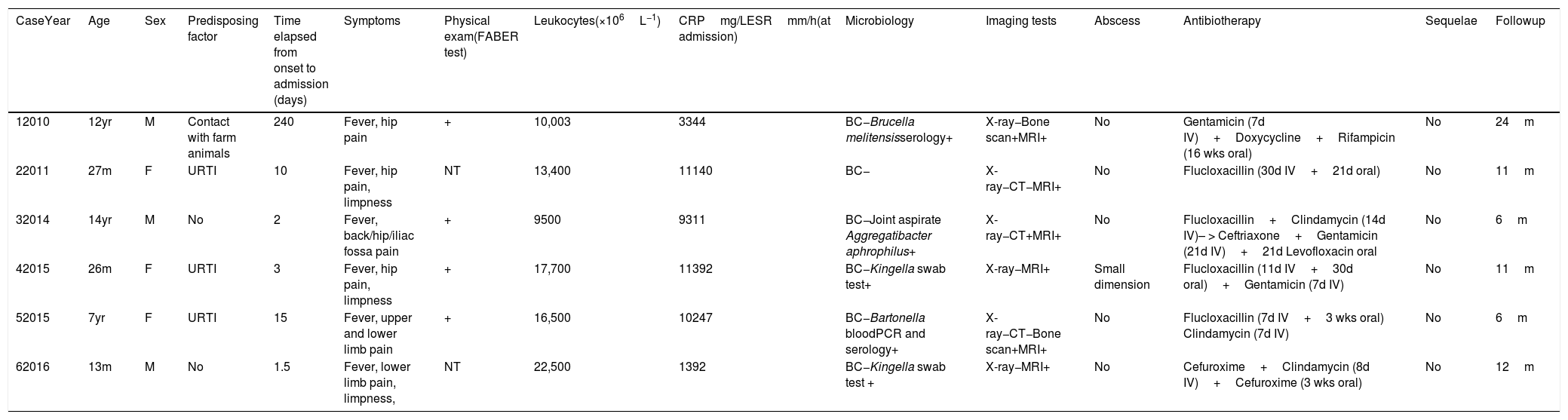
Epidemiological and clinical data; treatment and outcome of patients with pyogenic sacroiliitis (January 2008–August 2016).
| CaseYear | Age | Sex | Predisposing factor | Time elapsed from onset to admission (days) | Symptoms | Physical exam(FABER test) | Leukocytes(×106L−1) | CRPmg/LESRmm/h(at admission) | Microbiology | Imaging tests | Abscess | Antibiotherapy | Sequelae | Followup |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 12010 | 12yr | M | Contact with farm animals | 240 | Fever, hip pain | + | 10,003 | 3344 | BC−Brucella melitensisserology+ | X-ray−Bone scan+MRI+ | No | Gentamicin (7d IV)+Doxycycline+Rifampicin (16 wks oral) | No | 24m |
| 22011 | 27m | F | URTI | 10 | Fever, hip pain, limpness | NT | 13,400 | 11140 | BC− | X-ray−CT−MRI+ | No | Flucloxacillin (30d IV+21d oral) | No | 11m |
| 32014 | 14yr | M | No | 2 | Fever, back/hip/iliac fossa pain | + | 9500 | 9311 | BC−Joint aspirate Aggregatibacter aphrophilus+ | X-ray−CT+MRI+ | No | Flucloxacillin+Clindamycin (14d IV)– > Ceftriaxone+Gentamicin (21d IV)+21d Levofloxacin oral | No | 6m |
| 42015 | 26m | F | URTI | 3 | Fever, hip pain, limpness | + | 17,700 | 11392 | BC−Kingella swab test+ | X-ray−MRI+ | Small dimension | Flucloxacillin (11d IV+30d oral)+Gentamicin (7d IV) | No | 11m |
| 52015 | 7yr | F | URTI | 15 | Fever, upper and lower limb pain | + | 16,500 | 10247 | BC−Bartonella bloodPCR and serology+ | X-ray−CT−Bone scan+MRI+ | No | Flucloxacillin (7d IV+3 wks oral) Clindamycin (7d IV) | No | 6m |
| 62016 | 13m | M | No | 1.5 | Fever, lower limb pain, limpness, | NT | 22,500 | 1392 | BC−Kingella swab test + | X-ray−MRI+ | No | Cefuroxime+Clindamycin (8d IV)+Cefuroxime (3 wks oral) | No | 12m |
BC, blood culture; CPR, C-reactive protein; CT, computed tomography; ESR, erythrocyte sedimentation rate; IV, intravenous; F, female; M, male; MRI, magnetic resonance imaging; PCR, polymerase chain reaction; URTI, upper respiratory tract infection.
The findings of pelvic X-rays were normal in all patients. A computed tomography (CT) scan was performed in 3 patients, and in one of them revealed a small subchondral sequestrum of the lower third of the sacroiliac joint that was probably secondary to a subchondral osteomyelitis foci with cortical disruption and subsequent joint involvement. Skeletal scintigraphy was performed in 2 patients, both with sacroiliac increased uptake. The findings of T2-weighted and gadolinium-enhanced T1-weighted magnetic resonance imaging were abnormal in all patients, with signal hyperintensity in the sacroiliac joint line and adjacent muscles. In one patient (case 3), the gadolinium-enhanced image also revealed a small intra-articular abscess.
When we compared children aged less than 4 years with older children, we found that they presented more often with a limp or difficulty bearing weight, received an earlier diagnosis (4.8 vs. 85.7 days), had higher mean leucocyte counts and CRP levels at admission, and had a shorter treatment duration (42 vs. 65 days). In younger infants, testing of oropharyngeal samples with PCR identified K. kingae in 2 patients, while no causative agent was identified in the third one (Table 1). In the older group, different bacteria were identified in each case: Aggregatibacter aphrophilus (n=1) by joint fluid culture, and Bartonella henselae (n=1) and Brucella melitensis (n=1) by enzyme-linked immunoassay (ELISA). In older children, antimicrobial regimens were adjusted to target the specific aetiological agent—doxycycline plus rifampicin (16 weeks) for brucellosis and ceftriaxone followed by levofloxacin (6 weeks) for A. aphrophilus—based on susceptibility tests. For B. henselae, the antibiotic treatment was not adjusted because the patient exhibited complete clinical and radiological resolution on flucloxacillin and gentamicin. All patients showed a favourable clinical response and were free from sequelae during the follow-up (average, 11.7 months) (Table 1).
DiscussionWe have described six cases of sacroiliitis, which corresponded to 0.67 cases per year. This incidence is comparable to the one in a larger series published by Donzelli et al., who reported 16 cases in a review spanning of 25 years (0.64cases/year). Also consistently with their series, we noticed a biphasic age distribution, with 3 children aged less than 4 years and 3 aged 7–14 years.
Due to the nonspecificity of the clinical features and laboratory findings of PSI, it is important to maintain a high level of suspicion for this diagnosis. Specific tests for the sacroiliac joint are frequently positive,2–4 but they are used unevenly in the physical examination due to the low level of suspicion.1 An increased awareness of the importance of this test in the systematic evaluation of back pain complaints, especially in older children, could contribute to an earlier diagnosis. In very young children, however, the clinical assessment is particularly difficult and the FABER test rarely feasible, with limping and decreased weight bearing being the most frequent nonspecific complaints.7 In our series, however, the FABER test was positive in the 4 cases it was performed, including those of 2 young children.
The growing availability of MRI in recent years has improved the diagnostic process, with a reported sensitivity and specificity of 95% and 100%, respectively.1 This technique can achieve an earlier diagnosis without exposure to radiation, while offering a good visualisation of the complex anatomy of the sacroiliac joint and the ability to identify the presence of fluid in the sacroiliac joint, bone marrow oedema, soft tissue abscess and spinal involvement.1,6 Bone scintigraphy is less sensitive, especially when performed earlier in the course of disease, and cannot detect local abscesses.3,6,10
Performing specific tests for less frequent agents was essential in the identification of the causative microorganism. The reliability on blood cultures for identification of the causative agent has been widely questioned in the literature, as positive results rates range between 27% and 50%.2,4,6,10 Culture of joint fluid aspiration samples can be considered as an alternative, but its poor diagnosis performance and the risks associated with surgery and anaesthesia preclude its indication, especially in younger children.5,6 Indeed, in our series, all blood cultures were negative and S. aureus was not isolated from any samples, even though it is usually the most common causative agent in all series reported 2,4 and also in our hospital, for other osteoarticular infections (OAIs). Surprisingly, in case 3 A. aphrophilus was isolated from the synovial fluid. To our knowledge, there is only one other published case of sacroiliitis caused by this bacterium, which occurred in an adult patient.11 The optimal antibiotic regimen for this aetiological agent has not been established, although based on antimicrobial susceptibility testing, our patient was treated with intravenous ceftriaxone followed by oral levofloxacin and achieved clinical improvement.
K. kingae has emerged as a common cause of OAIs in children aged less than 4 years.9 Specific PCR testing in oropharyngeal samples has been considered a reliable method for detection of K. kingae in OAIs, particularly when direct synovial fluid aspiration is unfeasible. Although we could not rule out the possibility of carriage state, it is fair to assume that this was the etiologic agent of PSI.
Sacroiliitis is the predominant form of skeletal involvement in brucellosis, with an incidence that ranges between 4.8% and 48.7% in the paediatric population.12,13 Diagnosis is difficult due to the nonspecific clinical presentation and low sensitivity of blood cultures, especially in subacute and chronic presentations, with the overall positivity rate ranging from 15% to 70% despite the use of several enhancing techniques.14–16 Moreover, serological tests for brucellosis and more recently developed specific PCR assays have improved diagnosis sensitivity.16 Although this infection is currently less common in Portugal ,17 we have to keep it in mind, especially in rural areas, where there is contact with sheep through farming, and in insidious clinical presentations. According to most published guidelines, treatment with doxycycline plus rifampicin with gentamicin is successful.18,19
There is evidence that B. henselae can be involved in the aetiology of osteomyelitis.20,21 In these cases, blood and bone biopsy cultures typically remain sterile and the diagnosis depends on molecular amplification or serological techniques such as indirect fluorescence assay (IFA) and enzyme-linked immunoassay (ELISA), which are used to detect serum antibody to B. henselae.20 Seroconversion confirms infection, as ocurred in our case. However, by the time Bartonella was confirmed, our patient was already asymptomatic and the antibiotic treatment was not modified. Although a multidrug regimen with doxycycline plus rifampicin or cotrimoxazole has been recommended for Bartonella-related OAIs, it is possible that treatment with gentamicin contributed to this improvement.22,23
ConclusionDespite the small sample size of our study, its findings emphasize the low effectiveness of blood culture for diagnosis of paediatric SIP. Consequently, it also highlighted the need for a high level of suspicion for atypical agents and the early use of appropriate diagnostic methods, including imaging tests,antibody and PCR blood analysis, and the implementation of an effective antimicrobial therapy. This seems to be particularly important in older children, in whom we found a more nonspecific and indolent presentation, which ultimately resulted in delayed diagnosis and longer duration of treatment.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Arcângelo J, Norte Ramos S, Alves P, Tavares D, Gouveia C. Sacroileítis piógena: Lecciones aprendidas de una serie de casos atípicos. An Pediatr (Barc). 2019;91:42–46.
