
Acute respiratory tract infections (ARTIs) of a viral aetiology are common in the paediatric age group. Although the most prevalent infections in the winter are those caused by respiratory syncytial virus (RSV) or influenza viruses, the use of molecular amplification techniques has evinced that a considerable percentage of cases (20–40%) involve more than one virus, that is, are coinfections.1,2
The current evidence is insufficient to establish whether coinfection is associated with a higher morbidity or mortality, although both depend on the viruses involved.1,3 Given the current uncertainty that exists in regard to the clinical course of these infections, we thought it would be relevant to review the cases of coinfection that involved RSV and influenza viruses.
We analysed the prevalence of respiratory viruses in all patients aged less than 2 years with a suspected acute infection of the upper or lower respiratory tract that sought care in our emergency department in the 2014–2017 period. The method used for detection of respiratory viruses was a multiple RT-PCR assay (Anyplex™ RV16, Seegene, Korea) capable of simultaneously detecting and differentiating between 16 viruses.
We found 803 cases of influenza in the period under study, 515 cases of influenza A (64.1%) and 208 of influenza B (25.9%), as well as 992 cases of infection by RSV, 588 involving RSV subtype A (59.2%) and 404 subtype B (40.8%).
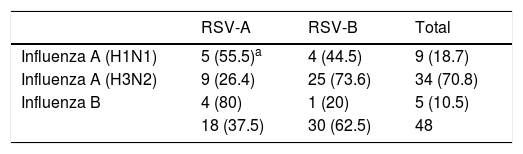
There were 48 cases of coinfection by RSV and influenza viruses (Table 1). These 48 cases amounted to 5.9% of detected cases of influenza, of which 43 (89.5%) corresponded to type A (8.3% of total cases of influenza A) and 5 (10.5%) to type B (2.4% of the total cases of influenza B). Of all cases of influenza A virus infection, 34 (79%) corresponded to subtype A(H3N2) and 9 (21%) to subtype A(H1N1)pdm09.
Distribution of viral coinfections detected in the period under study.
| RSV-A | RSV-B | Total | |
|---|---|---|---|
| Influenza A (H1N1) | 5 (55.5)a | 4 (44.5) | 9 (18.7) |
| Influenza A (H3N2) | 9 (26.4) | 25 (73.6) | 34 (70.8) |
| Influenza B | 4 (80) | 1 (20) | 5 (10.5) |
| 18 (37.5) | 30 (62.5) | 48 |
The cases of influenza and RSV coinfection amounted to 4.8% of the total detected cases of RSV, with 18 cases (37.5%) corresponding to subtype A (3% of the total RSV-A cases) and the other 30 cases (62.5%) to subtype B (7.4% of the total RSV-B cases).
Of all patients, 8 (16.6%) were aged 0–3 months, 4 (8.3%) 4–6 months, 16 (33.3%) 6–12 months, 7 (14.5%) 12–18 months and 13 (27.1%) 18–24 months; 58.3% of the cases occurred in infants aged less than 1 year. Boys amounted to 56.2% of the sample and girls to 43.8%. The distribution of cases by month was 43.7% in December, 25% in January, 14.5% in February, 12.5% in November and 4.1% in March.
The ARTI was a flu-like syndrome in 20 cases (41.6%), bronchiolitis in 15 (31.3%), bronchitis in 9 (18.7%) and pneumonia in 4 (8.3%). Eleven patients (22.9%) required hospital admission, and none of the patients died.
Coinfections by respiratory viruses is found in 20% to 40% of cases, although the percentage may reach up to 70% for certain viruses.1–3 In previous studies, we found that 32.5% of cases of influenza virus infection were coinfections with RSV,4,5 and up to 2014, RSV type A was most frequently involved in these cases.5 However, in the most recent seasons there has been a high incidence of RSV-B, amounting to nearly 58% of cases. This trend would explain the higher number of coinfections by influenza viruses and RSV-B that we found (62.5%). Furthermore, the most frequent influenza virus involved in these coinfections was type A(H3N2) (70.8%), the type that has predominated in nearly all recent seasons.
Although influenza B virus chiefly infects children, it corresponded to the smallest proportion of coinfections (10.5%). This could be due to the fact that infection by this virus typically occurs at older ages compared to RSV.4
From a clinical standpoint, a majority of patients (43.7%) had a flu-like presentation, which may suggest that an influenza virus was the direct cause of the ARTI, however, it is not possible to discriminate these 2 viruses based solely on clinical features, and the only aspect that can guide this differentiation is the epidemiological context. During the epidemic season, RSV may be isolated from respiratory samples of asymptomatic individuals; this carriage would be responsible for the transmission and spread of the infection, giving rise to seasonal outbreaks in the winter.1,3
In cases of bronchiolitis, it is difficult to establish which of the 2 viruses could be involved, although Reina et al.6 reported that in the 1999–2000 period, 52.9% of bronchiolitis cases in the winter season were caused by influenza A virus (H3N2), without detection of RSV.
Thus, it appears that the incidence of coinfection by influenza viruses and RSV is very low, while it is difficult to infer the direct role of each virus in the pathogenesis of ARTIs in infants aged less than 1 year.
Please cite this article as: Reina J, Dueñas J. Coinfecciones respiratorias entre los virus gripales y el virus respiratorio sincitial (2014-2017). An Pediatr (Barc). 2019;90:118–119.
