




Right atrial appendage enlargement is an infrequent disease characterised by the enlargement of the appendage in the absence of any other cardiac lesions.1 There are very few cases published in the literature, most of them in adults, and rarely diagnosed antenatally.2 The age of onset ranges from the foetal period to adulthood. The clinical presentation in the paediatric population is variable, and most patients are asymptomatic and diagnosed based on incidental findings. It is also variable in affected foetuses, ranging from the absence of symptoms to foetal hydrops due to severe tricuspid regurgitation.3 It is essential that it be diagnosed due to its potential complications: hard-to-control tachyarrhythmias, thromboembolic events, dyspnoea, sudden death or heart palpitations. Its natural history is still not well understood, and this poses barriers to reaching a consensus on its management, so that treatment must be personalised based on symptoms and serial echocardiographic findings. Some authors propose watchful waiting in asymptomatic patients, while others recommend oral anticoagulant therapy or surgical resection depending on the disease course to prevent complications.2
We present two cases of right atrial appendage enlargement diagnosed prenatally, and their course to date.
Case 1Patient aged 18 months in whom an aneurismal enlargement of the right atrium appendage was suspected prenatally, with echocardiography revealing an area of 4cm2 in the four-chamber view at 31.6 weeks’ gestational age, and no other family history of interest. The patient was born through elective caesarean delivery at 39 weeks’ gestational age and admitted for monitoring. There were no complications during labour or the perinatal period. Treatment with acetylsalicylic acid (ASA) was initiated and is still ongoing due to persistent significant enlargement. The size of the atrium has decreased gradually, with an area of 8cm2 at 4 months of chronological age and 5cm2 in the last echocardiographic control at age 18 months, which revealed no intra-auricular thrombi and a normal right atrium morphology (Fig. 1). The serial echocardiograms have not detected arrhythmias or other complications, and the patient has remained asymptomatic and with normal findings in physical examination throughout the followup.
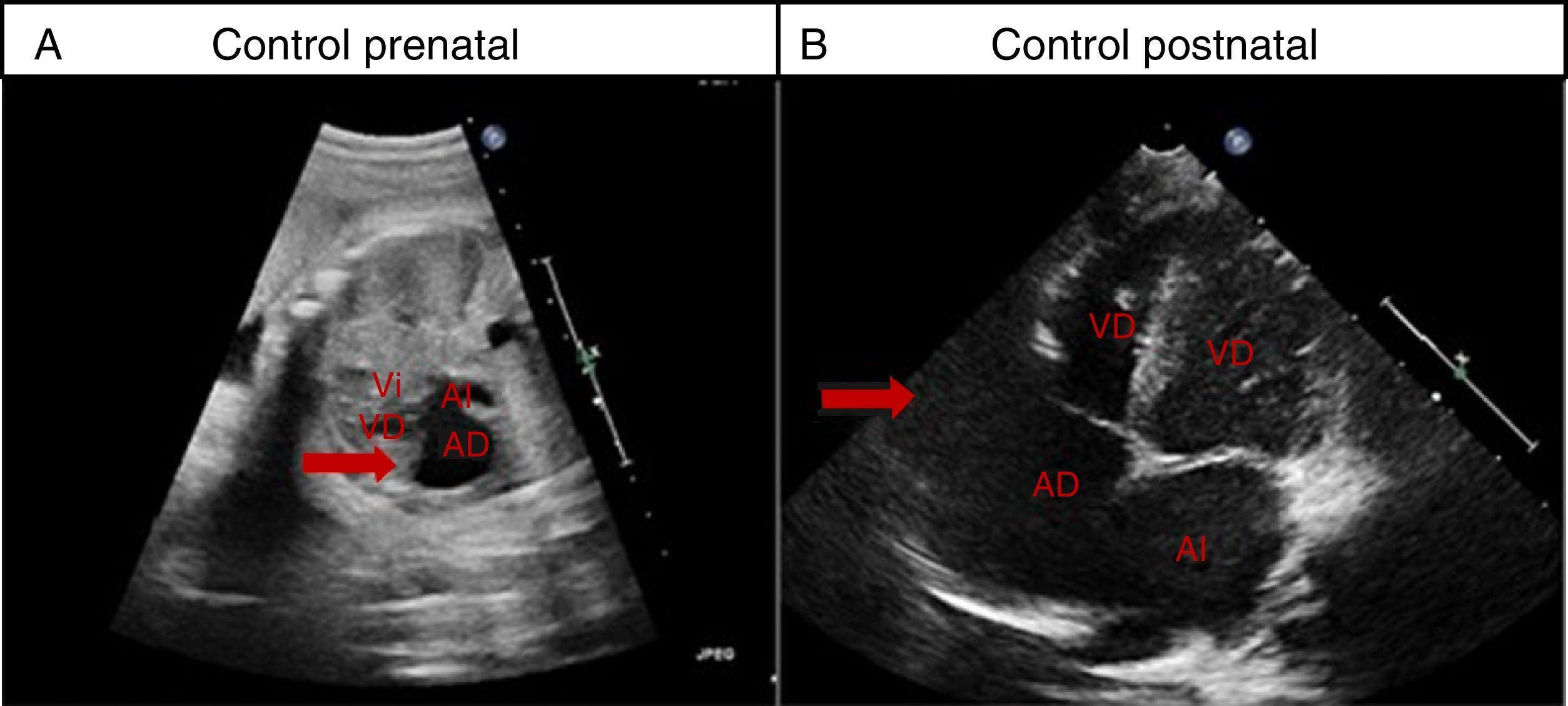
Case 1. Right atrial appendage enlargement. (A) Foetal ultrasound at 31 weeks’ gestation, arrow points at right atrial enlargement. (B) Ultrasound: last postnatal followup at 18 months of age showing enlargement of right atrial appendage 5cm2 in diameter (arrow). AD, right atrium; AI, left atrium; VD, right ventricle; VI, left ventricle.
Patient aged 15 months with right atrial appendage enlargement diagnosed prenatally at 20 weeks’ gestational age, with an area of 1.6cm2 detected in the four-chamber view at 35 weeks’ gestation. She was admitted to the hospital for twenty-four hours after an uncomplicated delivery at 40.1weeks’ gestation for observation and cardiac monitoring, and had no arrhythmia or other complications. The atrial appendage size has remained constant during the followup, with an area of 3.5cm2 observed in the four-chamber view. There has been no evidence of intra-auricular thrombi (Fig. 2). In this patient, given the absence of symptoms and complications, we adopted a watchful waiting approach and did not initiate treatment.
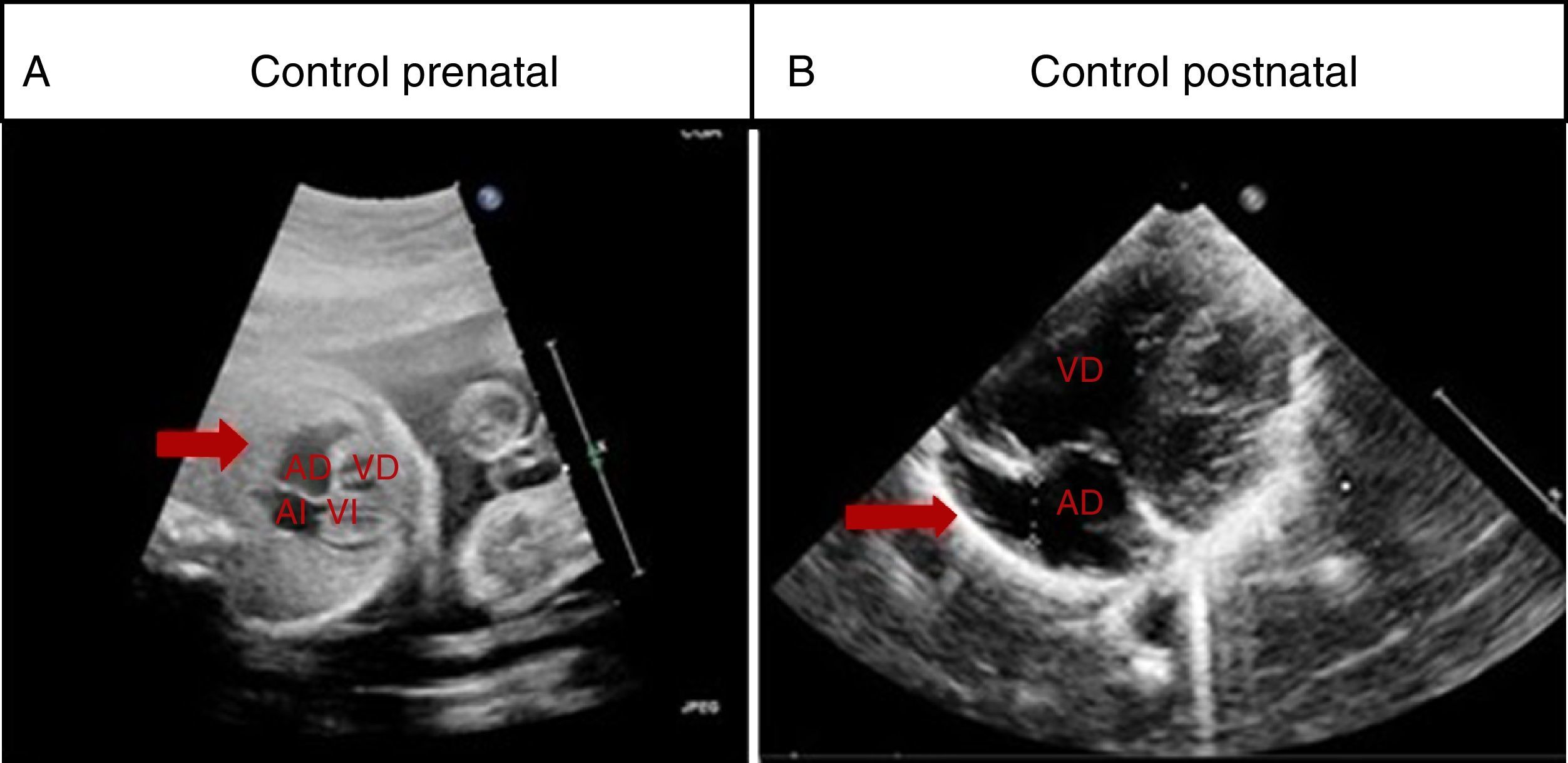
Case 2. Right atrial appendage enlargement. (A) Foetal ultrasound at 22 weeks’ gestation, arrow points at right atrial enlargement. (B) Postnatal follow-up ultrasound at 1 year of life showing enlargement of the right atrial appendage 6mm in diameter (arrow). AD, right atrium; AI, left atrium; VD, right ventricle; VI, left ventricle.
In the literature, the cases of idiopathic right atrial appendage enlargement that are diagnosed prenatally are exceptional. Since this is a rare disease that can present with significant complications, its early diagnosis allows an assessment of its course and informing the family more thoroughly.
The idiopathic enlargement of the right atrial appendage can be confused with other cardiopathies, such as Ebstein anomaly4 or, as occurred in our case during early prenatal tests, with a pericardial cyst, which was ruled out at a later time. The differential diagnosis with Ebstein anomaly is easy if there is evidence of normal insertion of the tricuspid valve.
The postnatal diagnosis can be made by means of techniques such as transthoracic and transesophageal ultrasound, computed tomography and magnetic resonance imaging, although transthoracic echocardiography usually suffices for definitive diagnosis in the paediatric age group.5 Given the age of these patients and the optimal visualisation by means of transthoracic ultrasound to present, we have not needed other imaging tests that would require, at this time, the sedation or anaesthesia of the children, although they may be needed in the future.
Since the diagnosis was made prenatally in our patients and we performed serial echocardiograms, we could anticipate potential complications. We adopted a conservative approach at the outset due to the absence of symptoms, and in one case the extent of the enlargement eventually led to initiation of anticoagulant therapy, which is associated with few adverse effects. Depending on the course of the disease in each patient, and on a personalised basis, we will choose whether to maintain the conservative approach or use more invasive interventions, such as surgical excision.
The two cases presented here are exceptional because they were diagnosed before birth. This disease should be suspected when foetal echocardiography detects a right atrium-dependent dilation with no evidence of other possible causes. Its correct diagnosis makes it possible to provide appropriate follow-up care to prevent potential complications.
Please cite this article as: Cardiel Valiente L, Orden Rueda C, Ayerza Casas A, Palanca Arias D, Jiménez Montañés L. Dilatación de la orejuela derecha: diagnóstico prenatal y seguimiento postnatal. An Pediatr (Barc). 2016;84:337–339.
