

Clinical simulation has established itself as an essential educational tool in the health care field. Its main objective is to improve patient safety by promoting the acquisition of technical and nontechnical skills through the construction of a parallel reality that allows for the development of individuals, teams and organizations. It has been used in emergency care settings1 to train staff on the response to critical situations, which is particularly relevant in pediatrics, given their low incidence. Currently, simulation is being applied to a growing number of activities outside critical care.
The purpose of this editorial is to provide a summary of the key processes to consider in the design and implementation of simulation-based activities (SBAs).
Experiential learning as an educational toolThe theoretical model that supports SBAs is the experiential learning cycle described by Kolb and Kolb.2 This theory conceptualizes learning as a dynamic and cyclical four-stage process that is triggered by a concrete experience (in this case, a simulation scenario). The second stage is to observe and reflect critically on the experience. The third involves abstract conceptualization to develop theories or models to apply to new experiences (in an SBA, reflection and conceptualization take place in the discussion following the scenario). Last of all, the fourth stage involves active experimentation, in which the participant applies the theoretical models to new situations (simulated or real), which become new concrete experiences, thereby closing the circle. The strengths of experiential learning, which link theory with practice, allow adaptation to different learning styles and promote autonomy as well as critical reflection, making SBAs a very effective educational approach.
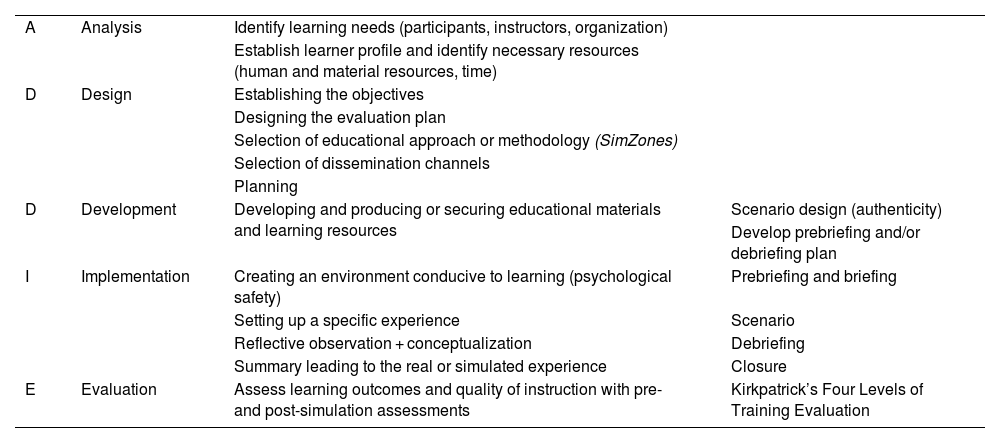
Simulation-based activities as an ongoing improvement processThe ADDIE model (Analysis, Design, Development, Implementation and Evaluation)3 offers a structured and systematic framework to design, develop and implement effective educational activities. Table 1 presents the ADDIE model applied to SBAs. To design a SBA that has an impact on learning in participants, a preliminary needs analysis should be conducted, using different methodologies, in addition to establishing specific, measurable, achievable and relevant objectives within a given time frame. Once the activity is developed and implemented, the process must be evaluated to assess whether the objectives were achieved and to identify areas for improvement for instructors or new needs among participants. Kirkpatrick’s Four Levels of Training Evaluation4 is one of the models most widely used for the purpose.
Stages of simulation-based learning with the ADDIE approach.
| A | Analysis | Identify learning needs (participants, instructors, organization) | |
| Establish learner profile and identify necessary resources (human and material resources, time) | |||
| D | Design | Establishing the objectives | |
| Designing the evaluation plan | |||
| Selection of educational approach or methodology (SimZones) | |||
| Selection of dissemination channels | |||
| Planning | |||
| D | Development | Developing and producing or securing educational materials and learning resources | Scenario design (authenticity) |
| Develop prebriefing and/or debriefing plan | |||
| I | Implementation | Creating an environment conducive to learning (psychological safety) | Prebriefing and briefing |
| Setting up a specific experience | Scenario | ||
| Reflective observation + conceptualization | Debriefing | ||
| Summary leading to the real or simulated experience | Closure | ||
| E | Evaluation | Assess learning outcomes and quality of instruction with pre- and post-simulation assessments | Kirkpatrick’s Four Levels of Training Evaluation |
The SimZones model proposed by Roussin y Weinstock5 is a system for organizing SBAs that takes into account the experience of participants and the learning objectives. It divides simulations into five zones (Fig. 1), of which the last one corresponds to learning in situ in the real-world work setting.

SimZones model for organizing simulation-based learning. Adapted from Roussin and Weinstock.5
In zone 0, learners are inexperienced, there is no instructor and the feedback is automatic: A surgeon learns a new laparoscopic technique using a specific simulator. Zone 1 simulations are for learning foundational technical skills: a group of residents learn how to perform orotracheal intubation. Zone 2 are used for acute situational instruction on technical or nontechnical skills: residents practicing the management of septic shock. The goals in these zones are related to the actions that need to be performed and how they need to be performed to achieve the expected outcomes.
In zone 3 simulations, the objectives involve evaluating the cognitive frames that affect decision-making when a team faces a complex situation. These SBAs promote the development and growth of expert care teams and are chiefly applied to native teams.
On the other hand, the debriefing is the intentional discussion that follows a simulation experience and is the linchpin of experiential learning. The SimZones model takes into account the level of experience of the learners and the type of learning objectives to select the approach to debriefing. In zone 0–2 simulations, a debriefing aimed at correcting actions without questioning the underlying assumptions is preferred, using a more instructional approach with inexperienced participants (zone 1) or a more reflective approach with more experienced participants (zone 2). Zone 3 simulations use a debriefing approach that involves questioning and modifying one's own mental models or scripts, promoting profound changes through reflective feedback and facilitator support. Thus, the SimZones model adjusts the type of debriefing according to the learners' experience, encouraging critical reflection and ongoing professional development.
Implementation of a simulation-based activityThe implementation of an SBA consists of four stages: prebriefing, briefing, scenario and debriefing. Prebriefing includes prior preparation, during which the purpose and objectives of the simulation, the ground rules for participation and the materials are explained. A key point that must be established during the prebriefing and maintained throughout the activity is psychological safety, which could be defined as the shared belief among team members that each of them can take risks without fear of being judged by the rest of the team or the facilitator. These components includes elements such as confidentiality, respect and curiosity.
Briefing is the specific introduction to the scenario and provides context to participants just before it begins. Both prebriefing and briefing are necessary for participants to become involved and to elicit mental, physical and emotional processes that are as similar as possible to a real-world situation.
The scenario is the specific experience that will be reflected upon and subsequently conceptualized. It includes elements that give it physical realism (perceived by the senses), conceptual realism (coherence of what happens in the scenario) and emotional realism (emotions similar to those of real-world practice), providing an experience that facilitates the interaction among participants that is as faithful a reflection of reality as possible.
Debriefing is the core and longest part of an SBA. In this stage, learners receive feedback to improve their skills. For it to be effective, it is structured in key phases:
- •
Reaction: participants expresses the feelings triggered by the scenario; this step helps release stress and prepare for analysis.
- •
Description: the simulation is recalled and summarized, including the challenges experienced in the scenario, to gain a clear and objective record of what took place. Participants are thus led to reflect on what occurred during the simulation.
- •
Analysis: recording of observations. Critical reflection is encouraged in order to identify successes and mistakes and build models or concepts that can be applied in the real world.
- •
Summary: key learnings are summarized and participants are encouraged to integrate what they have learned into real-world situations or future simulations.
Simulation-based activities offer a unique opportunity for teams to practice and evaluate their behavior in terms of teamwork and other nontechnical skills (leadership, communication, etc) while participating in realistic scenarios under conditions that are safe both for patients and the members of the team. Simulation is also a useful tool in the analysis of systems and the design of work protocols or spaces, as it helps narrow the gap between how the work is perceived and how it actually is.
