



Childhood obesity is inversely associated with household socioeconomic status in high-income countries. Our aim was to explore the association between childhood weight status and household socioeconomic status in Spain in relation to family characteristics, perceptions and lifestyle habits and the school environment.
MethodsWe performed a descriptive analysis of child weight status according to family socioeconomic factors and mediating variables based on data from the ALADINO 2019 study in a sample of 16,665 schoolchildren representative of the population aged 6–9 years in Spain.
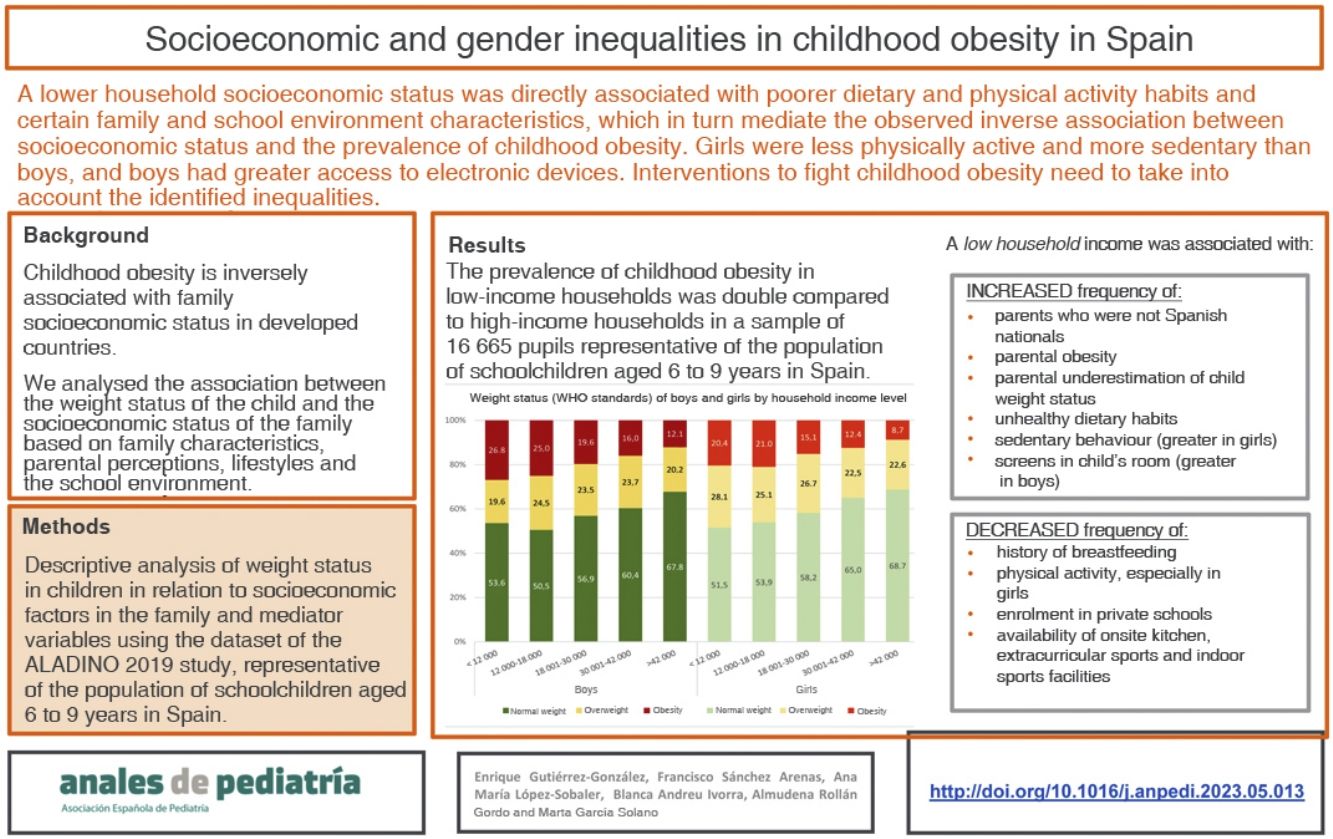
ResultsThe prevalence of childhood obesity in households with low socioeconomic status (26.8% boys; 20.4% girls) was, in both sexes, twice as high as in those with higher socioeconomic status (12.1% boys; 8.7% girls). Unhealthy eating habits, sedentary lifestyles (mainly in girls) and the presence of screens in the bedroom (more prevalent in boys) were more frequent in school-aged children from low-income households. On the other hand, in the most disadvantaged households, a history of breastfeeding and physical activity (especially in girls) were less frequent. Similarly, schools attended by children from low-income households were less likely to have their own kitchens and indoor gymnasiums or offer sports activities.
ConclusionA lower household socioeconomic status was associated with poorer dietary and physical activity habits and certain characteristics of the family and school environments that mediate the inverse association between household socioeconomic status and the prevalence of childhood obesity. Girls were less physically active and reported more sedentary lifestyles, while boys had greater access to screens. Interventions to combat childhood obesity should address the identified inequalities.
La obesidad infantil se asocia inversamente con el nivel socioeconómico familiar en países desarrollados. El objetivo es evaluar la asociación entre la situación ponderal infantil y el nivel socioeconómico familiar, según características familiares, percepciones, hábitos de vida y entorno escolar.
MetodologíaAnálisis descriptivo de la situación ponderal infantil según factores socioeconómicos familiares y variables mediadoras en el estudio ALADINO 2019, en una muestra de 16.665 escolares representativa de la población escolar de 6 a 9 años en España.
ResultadosLa prevalencia de obesidad infantil en hogares de bajo nivel socioeconómico (26,8% niños; 20,4% niñas) era, en ambos sexos, el doble de la de los de mayor nivel (12,1% niños; 8,7% niñas). En escolares de familias de baja renta eran más frecuentes hábitos alimentarios poco saludables, el sedentarismo (principalmente en niñas) y la presencia de pantallas en la habitación (más en niños). Por el contrario, en hogares más desfavorecidos eran menos frecuentes el antecedente de lactancia materna y la práctica de actividad física (especialmente en niñas). La disponibilidad de cocina propia, actividades deportivas y gimnasio cubierto en los centros era también menos habitual para los escolares de familias de menor renta.
ConclusionesUn menor nivel socioeconómico del hogar se asocia con peores hábitos alimentarios y de actividad física y ciertas características del entorno familiar y el escolar, que a su vez median la asociación inversa que existe entre el nivel socioeconómico y la prevalencia de obesidad infantil. Las niñas realizan menos actividad física y presentan más sedentarismo mientras que los niños tienen más acceso a pantallas. Las intervenciones para combatir la obesidad infantil deben contemplar las desigualdades identificadas.
Childhood overweight and obesity, jointly referred to as excess weight, are associated with multiple disorders and diseases in childhood, such as type 2 diabetes, high blood pressure or metabolic syndrome,1,2 as well as an increased probability of obesity and associated comorbidities (such as cardiovascular disease and certain forms of cancer) in adulthood.3
In recent decades, the prevalence of childhood excess weight has increased in Europe, including Spain.4 According to the 2018–2020 report of the Childhood Obesity Surveillance Initiative (COSI) of the World Health Organization (WHO) Regional Office for Europe, the prevalence of excess weight in school-aged children (ages 6–9 years) was 31% in boys and 28% in girls, while the prevalence for obesity was 14% in boys and 10% in girls.5 In Spain, the most recent round of the nationwide study of nutrition, physical activity, child development and obesity (known as ALADINO) of the Agencia Española de Seguridad Alimentaria y Nutrición (Spanish Food Safety and Nutrition Agency, AESAN), conducted in 2019, found a prevalence of excess weight of 41% in boys and 40% in girls and of obesity of 19% in boys and 15% in girls,6 with a decline and subsequent stabilization of childhood excess weight trends between 2011 and 2019, mainly on account of a decrease in the prevalence of overweight n boys. Given the magnitude and potential repercussions of this problem, it is a major public health challenge.7
Childhood obesity results from a complex interaction of factors, many of which are associated with the socioeconomic and cultural context, family background and school environment of the children.1,7 On the other, child poverty is a multifactorial phenomenon with a negative impact on dimensions as important as physical health, academic performance or emotional wellbeing.8 The child poverty rate in Spain is among the highest in Europe, with 27% of children and adolescents living in poverty in 2020.9
Childhood obesity and socioeconomic status are inversely correlated in high-income countries such as Spain, where childhood obesity is more frequent in families with lower versus higher socioeconomic status,10 as evinced by the different rounds of the ALADINO study6,11,12 or the National Health Survey.13 Yet, the evidence of the factors that mediate the association between childhood obesity and poverty in Spain is scarce.
The aim of our study was to assess the association between weight status in children aged 6–9 years in Spain and household socioeconomic variables from a sex-gender perspective, exploring factors related to household characteristics, lifestyle habits and the school environment that may mediate this association.
MethodsOverall design and sample of the ALADINO 2019 studyWe obtained the data to conduct the analysis from those collected in the ALADINO 2019 study, a cross-sectional, observational and descriptive study representative of the population of schoolchildren aged 6–9 years attending primary education (PE) schools in Spain. It corresponds to the fifth round of the COSI (the fourth in Spain), the methodology and design of which have been described in previous publications.11,12
We selected participants by random multi-stage cluster sampling categorised into 4 age groups (6, 7, 8 and 9 years), enrolled in years 1–4 of primary education. We selected PE schools at random, stratifying by autonomous community (AC) and municipality size, and then selected one classroom per school year per selected school by simple random sampling, including every student in the selected classrooms who attended school on the day of the visit, whose parents or legal guardians signed the informed consent form, and who agreed to undergo the necessary measurements. The resulting sample consisted of 16 665 students, with a uniform sex distribution, from 276 schools. The study was approved by the Ethics Committee of the Hospital Clínico San Carlos of Madrid.
Based on the models and methodological specifications of the COSI-EURO WHO surveys,14,15 we developed 3 questionnaires to be completed by the parents or legal guardians, the schools and the examiners. The weight, height and waist circumference were measured according to standardised procedures with properly calibrated equipment by qualified examiners.15,16
Study variablesTo assess the weight status of the children, we used the body mass index (BMI = weight [kg]/height2 [m2]) using the WHO growth standards as reference,17 and the waist-to-height ratio (WHtR), defining central obesity as a WHtR greater than 0.5.18
We considered the following socioeconomic variables: household income, parental educational attainment and parental employment. In relation to the family characteristics and history, we collected data on nationality, parental weight status and history of breastfeeding. As for perceptions and lifestyle habits, we analysed the parental perception of the child’s weight status, the results of the COSI questionnaire on unhealthy dietary habits,19 physical activity and sedentary behaviour and the number of screens in the child’s bedroom. The variables related to the school environment were the type of school (public, private or private but publicly funded), availability and type of food services, organization of extracurricular sports activities and availability of indoor sports facilities.
Analysis of results and statistical methodsSince some ACs increased their respective samples to obtain results representative for their region, there was an increase relative to the allocated proportion in the nationwide sample, so in our analysis we adjusted the results for sex, age and AC.
We conducted a descriptive analysis of the characteristics of the sample, the weight status of the schoolchildren in relation to variables related to the socioeconomic status of the family and of the mediator variables in relation to the income level. We categorised every variable and calculated absolute frequencies and percentages with 95% confidence intervals (CIs). We used the χ2 test to analyse the association between qualitative variables, considering differences significant if the P value was less than 0.05. We also made a quantitative analysis of the BMI and WHtR variables, calculating the median since the data did not follow a normal distribution, as determined with the Kolmogorov-Smirnov test. The statistical analysis was performed with the Stata package, version 16 (StataCorp LLC, Spain).
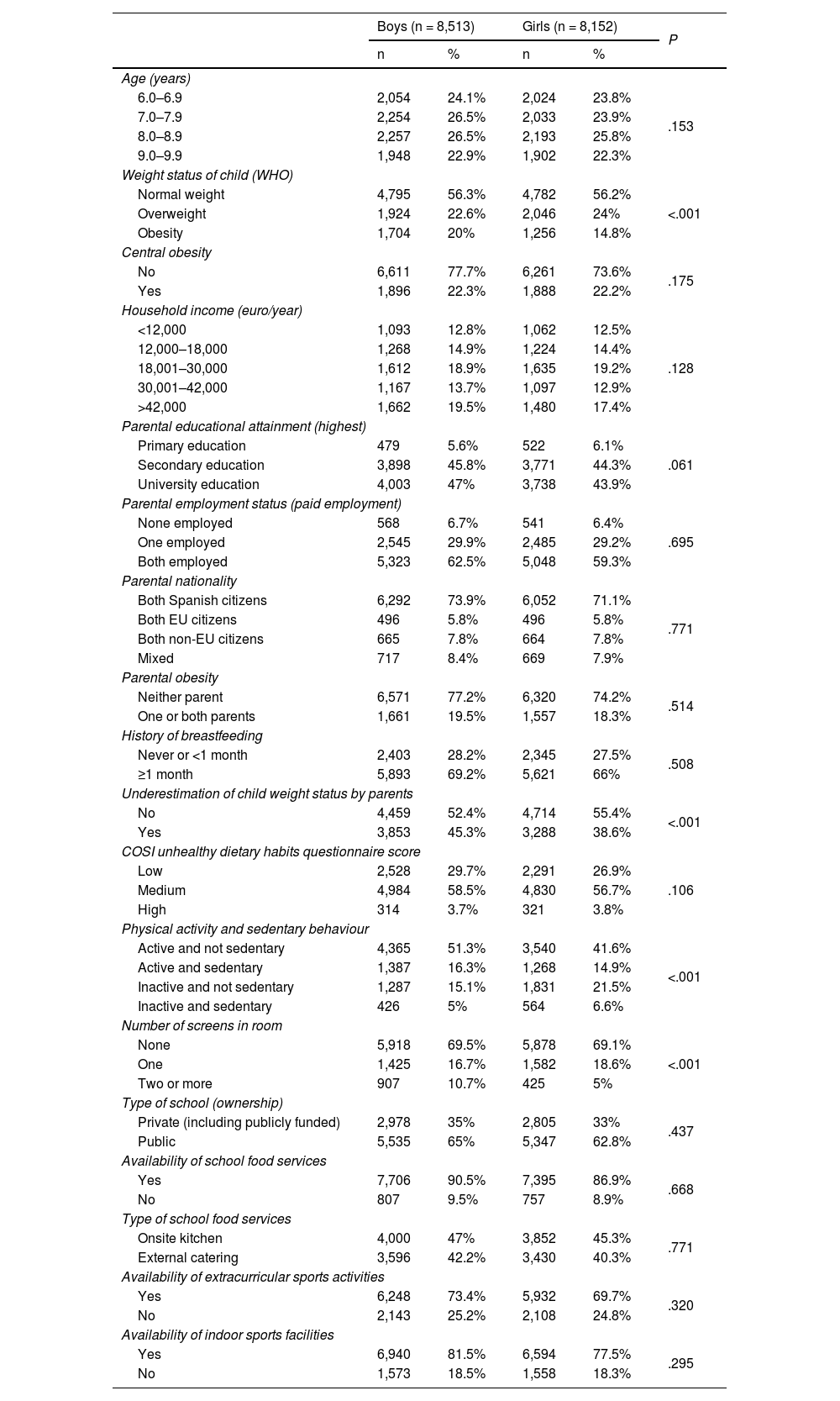
ResultsTable 1 summarises the general characteristics of the sample by sex. Compared to girls, boys had obesity more frequently, were more physically active and had more screens in their room, and their parents were more likely to underestimate their weight status; we did not find differences in any other variables based on sex.
Sociodemographic and family characteristics, lifestyle habits and school environment of participants of the ALADINO 2019 study by sex.
| Boys (n = 8,513) | Girls (n = 8,152) | P | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age (years) | |||||
| 6.0–6.9 | 2,054 | 24.1% | 2,024 | 23.8% | .153 |
| 7.0–7.9 | 2,254 | 26.5% | 2,033 | 23.9% | |
| 8.0–8.9 | 2,257 | 26.5% | 2,193 | 25.8% | |
| 9.0–9.9 | 1,948 | 22.9% | 1,902 | 22.3% | |
| Weight status of child (WHO) | |||||
| Normal weight | 4,795 | 56.3% | 4,782 | 56.2% | <.001 |
| Overweight | 1,924 | 22.6% | 2,046 | 24% | |
| Obesity | 1,704 | 20% | 1,256 | 14.8% | |
| Central obesity | |||||
| No | 6,611 | 77.7% | 6,261 | 73.6% | .175 |
| Yes | 1,896 | 22.3% | 1,888 | 22.2% | |
| Household income (euro/year) | |||||
| <12,000 | 1,093 | 12.8% | 1,062 | 12.5% | .128 |
| 12,000–18,000 | 1,268 | 14.9% | 1,224 | 14.4% | |
| 18,001–30,000 | 1,612 | 18.9% | 1,635 | 19.2% | |
| 30,001–42,000 | 1,167 | 13.7% | 1,097 | 12.9% | |
| >42,000 | 1,662 | 19.5% | 1,480 | 17.4% | |
| Parental educational attainment (highest) | |||||
| Primary education | 479 | 5.6% | 522 | 6.1% | .061 |
| Secondary education | 3,898 | 45.8% | 3,771 | 44.3% | |
| University education | 4,003 | 47% | 3,738 | 43.9% | |
| Parental employment status (paid employment) | |||||
| None employed | 568 | 6.7% | 541 | 6.4% | .695 |
| One employed | 2,545 | 29.9% | 2,485 | 29.2% | |
| Both employed | 5,323 | 62.5% | 5,048 | 59.3% | |
| Parental nationality | |||||
| Both Spanish citizens | 6,292 | 73.9% | 6,052 | 71.1% | .771 |
| Both EU citizens | 496 | 5.8% | 496 | 5.8% | |
| Both non-EU citizens | 665 | 7.8% | 664 | 7.8% | |
| Mixed | 717 | 8.4% | 669 | 7.9% | |
| Parental obesity | |||||
| Neither parent | 6,571 | 77.2% | 6,320 | 74.2% | .514 |
| One or both parents | 1,661 | 19.5% | 1,557 | 18.3% | |
| History of breastfeeding | |||||
| Never or <1 month | 2,403 | 28.2% | 2,345 | 27.5% | .508 |
| ≥1 month | 5,893 | 69.2% | 5,621 | 66% | |
| Underestimation of child weight status by parents | |||||
| No | 4,459 | 52.4% | 4,714 | 55.4% | <.001 |
| Yes | 3,853 | 45.3% | 3,288 | 38.6% | |
| COSI unhealthy dietary habits questionnaire score | |||||
| Low | 2,528 | 29.7% | 2,291 | 26.9% | .106 |
| Medium | 4,984 | 58.5% | 4,830 | 56.7% | |
| High | 314 | 3.7% | 321 | 3.8% | |
| Physical activity and sedentary behaviour | |||||
| Active and not sedentary | 4,365 | 51.3% | 3,540 | 41.6% | <.001 |
| Active and sedentary | 1,387 | 16.3% | 1,268 | 14.9% | |
| Inactive and not sedentary | 1,287 | 15.1% | 1,831 | 21.5% | |
| Inactive and sedentary | 426 | 5% | 564 | 6.6% | |
| Number of screens in room | |||||
| None | 5,918 | 69.5% | 5,878 | 69.1% | <.001 |
| One | 1,425 | 16.7% | 1,582 | 18.6% | |
| Two or more | 907 | 10.7% | 425 | 5% | |
| Type of school (ownership) | |||||
| Private (including publicly funded) | 2,978 | 35% | 2,805 | 33% | .437 |
| Public | 5,535 | 65% | 5,347 | 62.8% | |
| Availability of school food services | |||||
| Yes | 7,706 | 90.5% | 7,395 | 86.9% | .668 |
| No | 807 | 9.5% | 757 | 8.9% | |
| Type of school food services | |||||
| Onsite kitchen | 4,000 | 47% | 3,852 | 45.3% | .771 |
| External catering | 3,596 | 42.2% | 3,430 | 40.3% | |
| Availability of extracurricular sports activities | |||||
| Yes | 6,248 | 73.4% | 5,932 | 69.7% | .320 |
| No | 2,143 | 25.2% | 2,108 | 24.8% | |
| Availability of indoor sports facilities | |||||
| Yes | 6,940 | 81.5% | 6,594 | 77.5% | .295 |
| No | 1,573 | 18.5% | 1,558 | 18.3% | |
EU, European Union; WHO, World Health Organization.
The prevalence of obesity and overweight decreased as household income increased, a gradient that was more pronounced in obesity (Fig. 1). The prevalence of obesity in children of low-income households was 2.3 times greater in boys and 2.2 times greater in girls compared to higher-income households, while the prevalence of overweight was 1.2 times greater in girls of low-income households, without significant differences in boys. In general, for each income bracket, overweight was more frequent than obesity, except in children from low-income households, in whom obesity was more frequent (Appendix A, Supplemental Table A1).
 of participants in the ALADINO 2019 study by household income and sex of the child.")
The prevalence of central obesity in the lowest-income bracket nearly doubled the prevalence in the highest-income bracket in both boys and girls (Fig. 2). The assessment of the BMI and the WHtR as continuous variables also revealed an inverse association between both these variables and income level (Appendix A, Supplemental Figures A1 and A2).
 of participants in the ALADINO 2019 study by household income and sex of the child.")
In the analysis by parental educational attainment, the prevalence of obesity was nearly double in children of parents with low educational attainment compared to children of parents with a university education for both sexes (Appendix A, Supplemental Table A1). The trends for central obesity had the same direction but were not as pronounced. In relation to parental employment status, the prevalence of obesity in children of either sex was 1.4 times greater when neither parent was employed compared to when both parents had paid employment. In the case of central obesity, we found no differences in girls, but there were differences in boys (1.3 times increase) in the same direction (Appendix A, Supplemental Table A2).
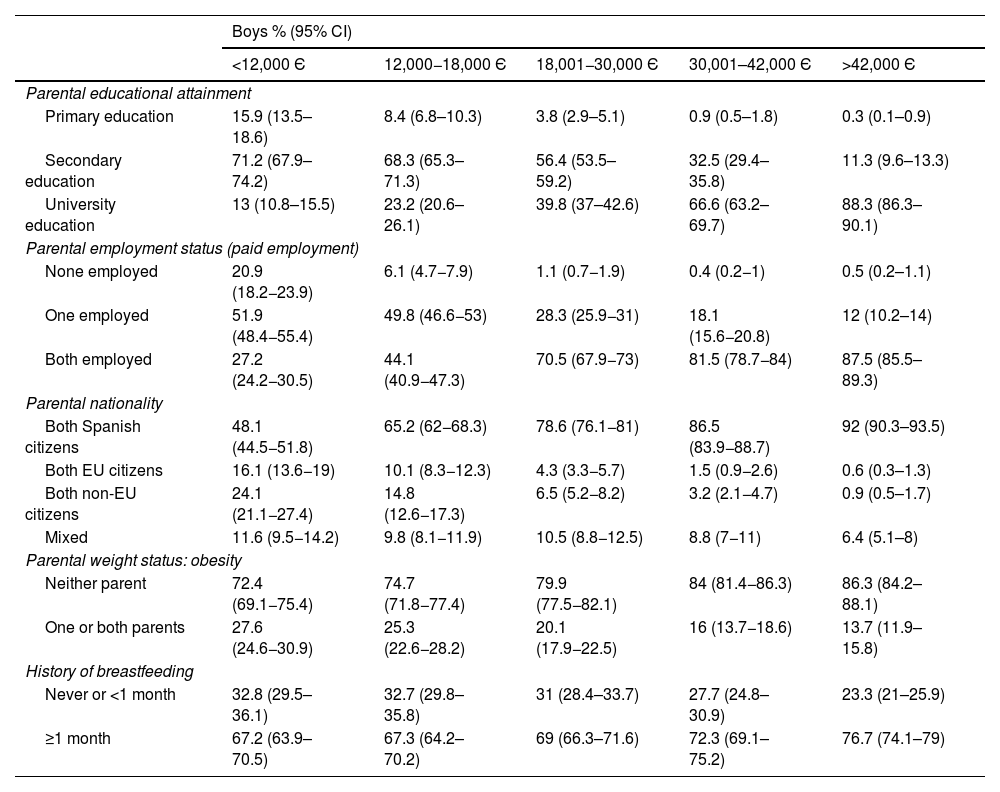
Association between family characteristics and household incomeFor both sexes, there was a direct association between parental educational attainment and household income, and the frequency of a university education was sevenfold in the highest income bracket compared to the lowest (Table 2). In most middle- or high-income households, one or both parents were employed, while in low-income households it was more frequent for a single parent to be employed.
Sociodemographic and family characteristics by annual household income and sex of the child in the ALADINO 2019 study participants.
| Boys % (95% CI) | |||||
|---|---|---|---|---|---|
| <12,000 Є | 12,000−18,000 Є | 18,001−30,000 Є | 30,001–42,000 Є | >42,000 Є | |
| Parental educational attainment | |||||
| Primary education | 15.9 (13.5–18.6) | 8.4 (6.8–10.3) | 3.8 (2.9–5.1) | 0.9 (0.5–1.8) | 0.3 (0.1–0.9) |
| Secondary education | 71.2 (67.9–74.2) | 68.3 (65.3–71.3) | 56.4 (53.5–59.2) | 32.5 (29.4–35.8) | 11.3 (9.6–13.3) |
| University education | 13 (10.8–15.5) | 23.2 (20.6–26.1) | 39.8 (37–42.6) | 66.6 (63.2–69.7) | 88.3 (86.3–90.1) |
| Parental employment status (paid employment) | |||||
| None employed | 20.9 (18.2−23.9) | 6.1 (4.7−7.9) | 1.1 (0.7−1.9) | 0.4 (0.2−1) | 0.5 (0.2–1.1) |
| One employed | 51.9 (48.4−55.4) | 49.8 (46.6−53) | 28.3 (25.9−31) | 18.1 (15.6−20.8) | 12 (10.2–14) |
| Both employed | 27.2 (24.2−30.5) | 44.1 (40.9−47.3) | 70.5 (67.9−73) | 81.5 (78.7−84) | 87.5 (85.5–89.3) |
| Parental nationality | |||||
| Both Spanish citizens | 48.1 (44.5−51.8) | 65.2 (62−68.3) | 78.6 (76.1−81) | 86.5 (83.9−88.7) | 92 (90.3–93.5) |
| Both EU citizens | 16.1 (13.6−19) | 10.1 (8.3−12.3) | 4.3 (3.3−5.7) | 1.5 (0.9−2.6) | 0.6 (0.3–1.3) |
| Both non-EU citizens | 24.1 (21.1−27.4) | 14.8 (12.6−17.3) | 6.5 (5.2−8.2) | 3.2 (2.1−4.7) | 0.9 (0.5–1.7) |
| Mixed | 11.6 (9.5−14.2) | 9.8 (8.1−11.9) | 10.5 (8.8−12.5) | 8.8 (7−11) | 6.4 (5.1–8) |
| Parental weight status: obesity | |||||
| Neither parent | 72.4 (69.1−75.4) | 74.7 (71.8−77.4) | 79.9 (77.5−82.1) | 84 (81.4−86.3) | 86.3 (84.2–88.1) |
| One or both parents | 27.6 (24.6−30.9) | 25.3 (22.6−28.2) | 20.1 (17.9−22.5) | 16 (13.7−18.6) | 13.7 (11.9–15.8) |
| History of breastfeeding | |||||
| Never or <1 month | 32.8 (29.5–36.1) | 32.7 (29.8–35.8) | 31 (28.4–33.7) | 27.7 (24.8–30.9) | 23.3 (21–25.9) |
| ≥1 month | 67.2 (63.9–70.5) | 67.3 (64.2–70.2) | 69 (66.3–71.6) | 72.3 (69.1–75.2) | 76.7 (74.1–79) |
| Girls % (95 % CI) | |||||
|---|---|---|---|---|---|
| <12,000 Є | 12,000−18,000 Є | 18,001−30,000 Є | 30,001−42,000 Є | >42,000 Є | |
| Parental educational attainment | |||||
| Primary education | 20.8 (18.1−23.9) | 9.8 (8.1−11.9) | 3.7 (2.7−5) | 1.3 (0.7−2.5) | 0.4 (0.1−1) |
| Secondary education | 66.7 (63.3−70) | 70.2 (67.1−73.1) | 55.5 (52.6−58.3) | 32.2 (29−35.6) | 12.4 (10.6−14.6) |
| University education | 12.4 (10.3−15) | 20 (17.5−22.7) | 40.8 (38−43.7) | 66.4 (63−69.7) | 87.2 (85−89.1) |
| Parental employment status (paid employment) | |||||
| None employed | 20.8 (18−23.9) | 4.1 (3−5.6) | 1.4 (0.8−2.2) | 1.2 (0.6−2.4) | 0.7 (0.3−1.5) |
| One employed | 52 (48.3−55.6) | 53 (49.8−56.3) | 29.9 (27.4−32.6) | 16.6 (14.2−19.3) | 11 (9.2−13.1) |
| Both employed | 27.2 (24−30.6) | 42.8 (39.7−46.1) | 68.7 (66−71.3) | 82.2 (79.4−84.6) | 88.3 (86.2−90.1) |
| Parental nationality | |||||
| Both Spanish citizens | 51.6 (47.9−55.3) | 64.8 (61.6−67.9) | 79.2 (76.7−81.5) | 90.2 (87.9−92.1) | 91.5 (89.6−93) |
| Both EU citizens | 14 (11.6−16.7) | 10.8 (8.9−13) | 4.9 (3.7−6.3) | 0.8 (0.4−1.8) | 1 (0.6−1.8) |
| Both non-EU citizens | 22.4 (19.4−25.6) | 13.9 (11.7−16.4) | 6.1 (4.8−7.6) | 2.4 (1.5−3.8) | 1.2 (0.7−2.1) |
| Mixed | 12.1 (9.9−14.7) | 10.5 (8.6−12.8) | 9.9 (8.3−11.8) | 6.6 (5−8.5) | 6.3 (4.9−7.9) |
| Parental weight status: obesity | |||||
| Neither parent | 76.9 (73.7−79.8) | 72.8 (69.8−75.6) | 80.5 (78.1−82.7) | 84 (81.3−86.4) | 86.2 (83.9−88.2) |
| One or both parents | 23.1 (20.2−26.3) | 27.2 (24.4−30.2) | 19.5 (17.3−21.9) | 16 (13.6−18.7) | 13.8 (11.8−16.1) |
| History of breastfeeding | |||||
| Never or <1 month | 32.9 (29.6−36.4) | 30.1 (27.2−33.2) | 33.9 (31.2−36.7) | 26.7 (23.7−30) | 24.4 (21.9−27.2) |
| ≥1 month | 67.1 (63.6−70.4) | 69.9 (66.8−72.8) | 66.1 (63.3−68.8) | 73.3 (70−76.3) | 75.6 (72.8−78.1) |
CI, confidence interval; EU, European Union.
On the other hand, in the highest-income bracket, 92% of schoolchildren had Spanish parents, a percentage that nearly doubled the percentage in the lowest-income bracket. The probability of having at least one obese parent was greater in low-income households (2.1 times greater in boys and 1.7 in girls) compared to high-income households. The history of breastfeeding was 1.1 times more frequent in boys and girls from high-income households compared to children from low-income households.
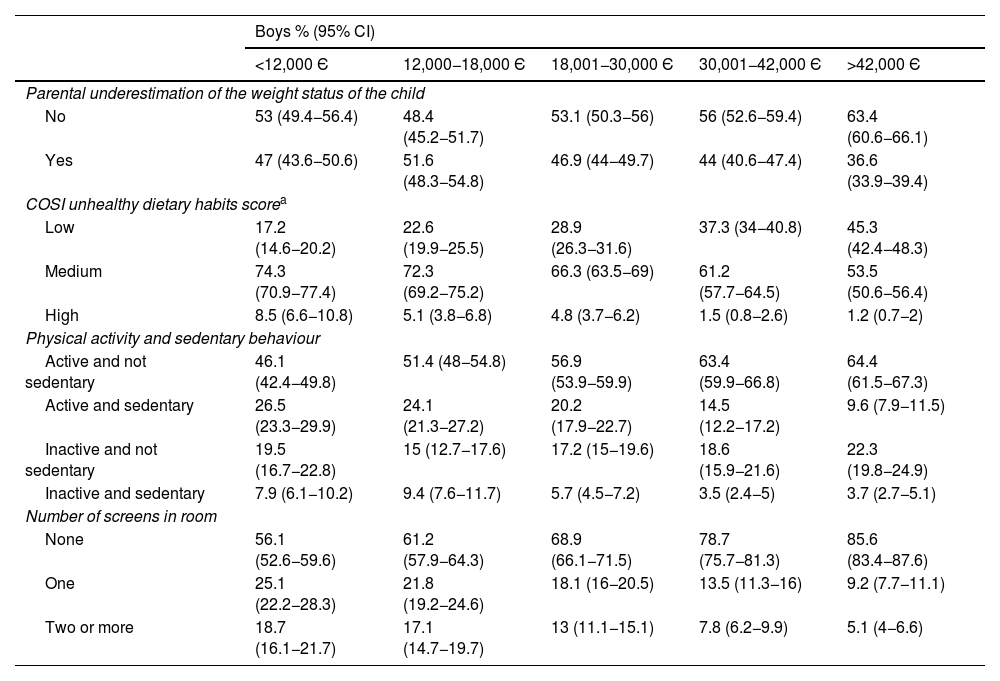
Association between perceptions and lifestyle habits and household incomeParents of low socioeconomic status were more likely to underestimate the weight status of schoolchildren compared to those of high socioeconomic status (Table 3). We also found an inverse association between the score in the COSI questionnaire of dietary habits and income: unhealthy dietary habits (higher scores) were 6 times more prevalent in schoolchildren from low-income households compared to high-income households.
Parental perceptions and schoolchildren habits by income level and child sex in the ALADINO 2019 sample.
| Boys % (95% CI) | |||||
|---|---|---|---|---|---|
| <12,000 Є | 12,000−18,000 Є | 18,001−30,000 Є | 30,001−42,000 Є | >42,000 Є | |
| Parental underestimation of the weight status of the child | |||||
| No | 53 (49.4−56.4) | 48.4 (45.2−51.7) | 53.1 (50.3−56) | 56 (52.6−59.4) | 63.4 (60.6−66.1) |
| Yes | 47 (43.6−50.6) | 51.6 (48.3−54.8) | 46.9 (44−49.7) | 44 (40.6−47.4) | 36.6 (33.9−39.4) |
| COSI unhealthy dietary habits scorea | |||||
| Low | 17.2 (14.6−20.2) | 22.6 (19.9−25.5) | 28.9 (26.3−31.6) | 37.3 (34−40.8) | 45.3 (42.4−48.3) |
| Medium | 74.3 (70.9−77.4) | 72.3 (69.2−75.2) | 66.3 (63.5−69) | 61.2 (57.7−64.5) | 53.5 (50.6−56.4) |
| High | 8.5 (6.6−10.8) | 5.1 (3.8−6.8) | 4.8 (3.7−6.2) | 1.5 (0.8−2.6) | 1.2 (0.7−2) |
| Physical activity and sedentary behaviour | |||||
| Active and not sedentary | 46.1 (42.4−49.8) | 51.4 (48−54.8) | 56.9 (53.9−59.9) | 63.4 (59.9−66.8) | 64.4 (61.5−67.3) |
| Active and sedentary | 26.5 (23.3−29.9) | 24.1 (21.3−27.2) | 20.2 (17.9−22.7) | 14.5 (12.2−17.2) | 9.6 (7.9−11.5) |
| Inactive and not sedentary | 19.5 (16.7−22.8) | 15 (12.7−17.6) | 17.2 (15−19.6) | 18.6 (15.9−21.6) | 22.3 (19.8−24.9) |
| Inactive and sedentary | 7.9 (6.1−10.2) | 9.4 (7.6−11.7) | 5.7 (4.5−7.2) | 3.5 (2.4−5) | 3.7 (2.7−5.1) |
| Number of screens in room | |||||
| None | 56.1 (52.6−59.6) | 61.2 (57.9−64.3) | 68.9 (66.1−71.5) | 78.7 (75.7−81.3) | 85.6 (83.4−87.6) |
| One | 25.1 (22.2−28.3) | 21.8 (19.2−24.6) | 18.1 (16−20.5) | 13.5 (11.3−16) | 9.2 (7.7−11.1) |
| Two or more | 18.7 (16.1−21.7) | 17.1 (14.7−19.7) | 13 (11.1−15.1) | 7.8 (6.2−9.9) | 5.1 (4−6.6) |
| Girls % (95 % CI) | |||||
|---|---|---|---|---|---|
| <12,000 Є | 12,000−18,000 Є | 18,001−30,000 Є | 30,001−42,000 Є | >42,000 Є | |
| Parental underestimation of the weight status of the child | |||||
| No | 50.9 (47.3−54.5) | 56.2 (53−59.4) | 57.5 (54.6−60.3) | 66.2 (62.8−69.5) | 67.1 (64.2−69.9) |
| Yes | 49.1 (45.5−52.7) | 43.8 (40.6−47) | 42.5 (39.7−45.4) | 33.8 (30.5−37.2) | 32.9 (30.1−35.8) |
| COSI unhealthy dietary habits scorea | |||||
| Low | 18.7 (15.8−21.9) | 23.2 (20.4−26.2) | 25.4 (23−28.1) | 35.4 (32−38.9) | 46.9 (43.8−50.1) |
| Medium | 70.9 (67.2−74.3) | 71.1 (67.9−74.1) | 69.8 (67−72.4) | 62.1 (58.5−65.5) | 51.3 (48.2−54.4) |
| High | 10.4 (8.2−13) | 5.7 (4.3−7.5) | 4.8 (3.7−6.3) | 2.5 (1.6−4) | 1.7 (1.1−2.8) |
| Physical activity and sedentary behaviour | |||||
| Active and not sedentary | 38.3 (34.6−42) | 43.1 (39.7−46.5) | 47.8 (44.8−50.8) | 53.4 (49.7−57.1) | 53.5 (50.3−56.7) |
| Active and sedentary | 26.6 (23.3−30.1) | 25.5 (22.6−28.6) | 18.7 (16.5−21.3) | 12.9 (10.6−15.6) | 7.9 (6.3−9.8) |
| Inactive and not sedentary | 25.3 (22.1−28.9) | 20.6 (18−23.5) | 24.5 (21.9−27.2) | 26.7 (23.5−30.1) | 34.1 (31.1−37.2) |
| Inactive and sedentary | 9.8 (7.8−12.3) | 10.8 (8.8−13.3) | 9 (7.4−10.9) | 7.1 (5.4−9.2) | 4.5 (3.4−6.1) |
| Number of screens in room | |||||
| None | 65 (61.4−68.5) | 61.5 (58.3−64.7) | 71.8 (69.2−74.4) | 82.5 (79.6−85.1) | 87.1 (84.9−89) |
| One | 26.2 (23.1−29.6) | 30.6 (27.7−33.8) | 22.6 (20.3−25.1) | 13.5 (11.2−16.1) | 11.1 (9.3−13.2) |
| Two or more | 8.8 (6.9−11.1) | 7.8 (6.2−9.8) | 5.5 (4.4−7) | 4 (2.8−5.7) | 1.8 (1.2−2.9) |
CI, confidence interval; COSI, Childhood Obesity Surveillance Initiative.
COSI unhealthy dietary habits score: one point given for each of the contemplated unhealthy dietary habits (skipping breakfast, failure to consume fruit daily, failure to consume vegetables daily, consumption of sugary drinks 4 or more times a week, consumption of sweet snacks four or more times a week, consumption of salty snacks four or more times a week). The possible total score ranges from 0 to 6, where 0 is healthiest and 6 least healthy. We categorised the score as low (0–1 points), medium (2–3 points) and high (4–6 points).
Physical activity and sedentary behaviour were directly and inversely associated, respectively, to household income level: the most sedentary and least physically active children were more likely to come from lower-income households. In every income bracket, the frequency of physical activity and lack of sedentary behaviour was about 10 points higher in boys compared to girls.
The number of screens in the student’s room was inversely correlated to income: having 2 or more screens in the room was nearly 4 times more frequent in boys and 5 times more frequent in girls from low-income households, compared to high-income households. We also ought to highlight that the presence of electronic devices in the room was more common in boys than girls.
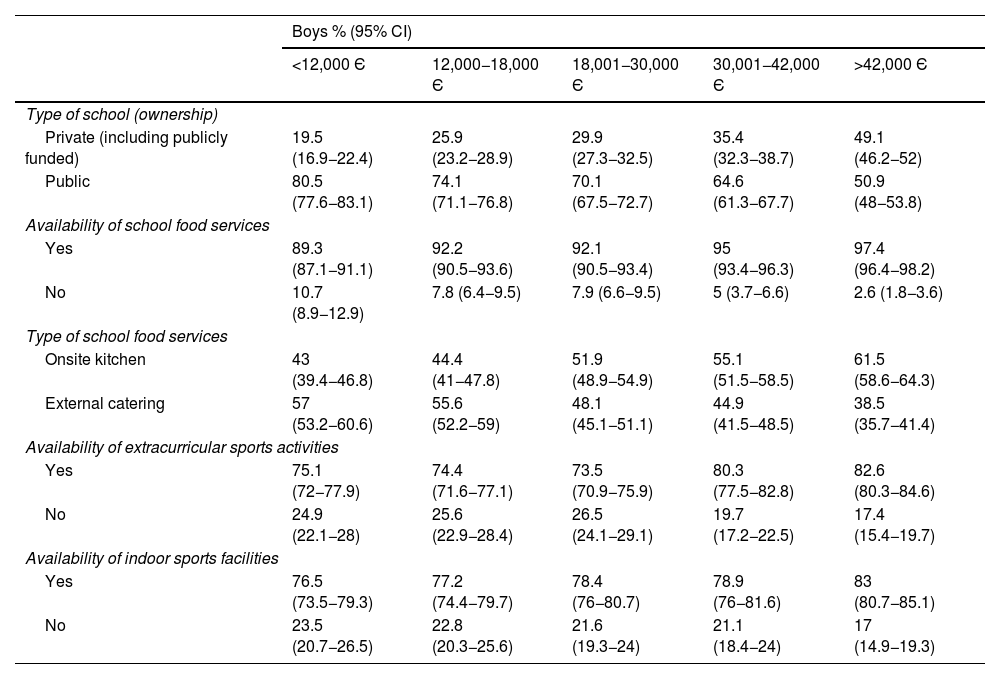
Association between school characteristics and household incomeAttendance to private or publicly funded private schools was twice as frequent in students from high-income homes compared to low-income homes (Table 4). Access to school lunch services and attendance to schools where the food was cooked on-site versus brought by a catering service were more frequent among students from high-income compared to low-income households (Table 4). Similarly, attendance to schools that organised sports activities or with indoor sports facilities was more frequent in students of high socioeconomic status.
Characteristics of the school environment by income level and child sex in the ALADINO 2019 sample.
| Boys % (95% CI) | |||||
|---|---|---|---|---|---|
| <12,000 Є | 12,000−18,000 Є | 18,001−30,000 Є | 30,001−42,000 Є | >42,000 Є | |
| Type of school (ownership) | |||||
| Private (including publicly funded) | 19.5 (16.9−22.4) | 25.9 (23.2−28.9) | 29.9 (27.3−32.5) | 35.4 (32.3−38.7) | 49.1 (46.2−52) |
| Public | 80.5 (77.6−83.1) | 74.1 (71.1−76.8) | 70.1 (67.5−72.7) | 64.6 (61.3−67.7) | 50.9 (48−53.8) |
| Availability of school food services | |||||
| Yes | 89.3 (87.1−91.1) | 92.2 (90.5−93.6) | 92.1 (90.5−93.4) | 95 (93.4−96.3) | 97.4 (96.4−98.2) |
| No | 10.7 (8.9−12.9) | 7.8 (6.4−9.5) | 7.9 (6.6−9.5) | 5 (3.7−6.6) | 2.6 (1.8−3.6) |
| Type of school food services | |||||
| Onsite kitchen | 43 (39.4−46.8) | 44.4 (41−47.8) | 51.9 (48.9−54.9) | 55.1 (51.5−58.5) | 61.5 (58.6−64.3) |
| External catering | 57 (53.2−60.6) | 55.6 (52.2−59) | 48.1 (45.1−51.1) | 44.9 (41.5−48.5) | 38.5 (35.7−41.4) |
| Availability of extracurricular sports activities | |||||
| Yes | 75.1 (72−77.9) | 74.4 (71.6−77.1) | 73.5 (70.9−75.9) | 80.3 (77.5−82.8) | 82.6 (80.3−84.6) |
| No | 24.9 (22.1−28) | 25.6 (22.9−28.4) | 26.5 (24.1−29.1) | 19.7 (17.2−22.5) | 17.4 (15.4−19.7) |
| Availability of indoor sports facilities | |||||
| Yes | 76.5 (73.5−79.3) | 77.2 (74.4−79.7) | 78.4 (76−80.7) | 78.9 (76−81.6) | 83 (80.7−85.1) |
| No | 23.5 (20.7−26.5) | 22.8 (20.3−25.6) | 21.6 (19.3−24) | 21.1 (18.4−24) | 17 (14.9−19.3) |
| Girls % (95% CI) | |||||
|---|---|---|---|---|---|
| <12,000 Є | 12,000−18,000 Є | 18,001−30,000 Є | 30,001−42,000 Є | >42,000 Є | |
| Type of school (ownership) | |||||
| Private (including publicly funded) | 21.4 (18.6−24.5) | 23.2 (20.6−26.1) | 30.8 (28.2−33.5) | 34.2 (31−37.6) | 47.8 (44.7−50.8) |
| Public | 78.6 (75.5−81.4) | 76.8 (73.9−79.4) | 69.2 (66.5−71.8) | 65.8 (62.4−69) | 52.2 (49.2−55.3) |
| Availability of school food services | |||||
| Yes | 92.3 (90.4−93.8) | 89.2 (87.2−91) | 93.6 (92.1−94.8) | 94.3 (92.5−95.7) | 97 (95.9−97.8) |
| No | 7.7 (6.2−9.6) | 10.8 (9−12.8) | 6.4 (5.2−7.9) | 5.7 (4.3−7.5) | 3 (2.2−4.1) |
| Type of school food services | |||||
| Onsite kitchen | 45.1 (41.4−48.9) | 46.1 (42.6−49.6) | 52.7 (49.7−55.7) | 55.1 (51.4−58.7) | 60.7 (57.6−63.7) |
| External catering | 54.9 (51.1−58.6) | 53.9 (50.4−57.4) | 47.3 (44.3−50.3) | 44.9 (41.3−48.6) | 39.3 (36.3−42.4) |
| Availability of extracurricular sports activities | |||||
| Yes | 73.2 (70−76.2) | 76.3 (73.5−78.9) | 74.6 (72.1−77) | 79 (76−81.7) | 81.6 (79.1−83.8) |
| No | 26.8 (23.8−30) | 23.7 (21.1−26.5) | 25.4 (23−27.9) | 21 (18.3−24) | 18.4 (16.2−20.9) |
| Availability of indoor sports facilities | |||||
| Yes | 75.5 (72.4−78.4) | 77.3 (74.5−79.9) | 76.7 (74.1−79) | 79.2 (76.2−81.9) | 83.3 (80.9−85.5) |
| No | 24.5 (21.6−27.6) | 22.7 (20.1−25.5) | 23.3 (21−25.9) | 20.8 (18.1−23.8) | 16.7 (14.5−19.1) |
CI, confidence interval.
In our study, we made a detailed analysis of the inverse association between childhood obesity and overweight, on one hand, and socioeconomic status, on the other, considering several mediating factors, thus offering a thorough and representative nationwide analysis of the social and gender gradient of weight status in the paediatric population and associated environmental variables for the first time.
The inverse gradient observed between excess weight (both obesity and overweight) and socioeconomic status, which was more evident for obesity than for overweight and for girls than for boys, was consistent with the findings of other studies conducted in Spain13 and at the international level.20 In addition, the data from the ALADINO study show diverging trends based on socioeconomic status: between 201511 and 2019,6 the prevalence of overweight and of obesity increased in low-income households (by 0.9% and 0.5%, respectively) and the prevalence of overweight in middle-income households (by 1.2%), while in households in the highest income bracket, the prevalence of overweight decreased by 1.5% and the prevalence of obesity by 0.8%. These differing trends in weight status based on income level have also been observed in previous studies in Spain21 and other European countries.22
Our findings show that the association between poverty and obesity is not only present in schoolchildren, but also in their parents. A previous study conducted in Spain also found an increased risk of obesity in children whose parents (one or both) had obesity, and this intergenerational pattern was more pronounced in boys than in girls and in the households in the extremes of the income distribution by quartiles.21 We also found a direct association between income and the history of breastfeeding.23 In families of low socioeconomic status, this may be due to a lower maternal educational attainment and poorer working conditions.24,25
Another relevant finding was that parents perceived the weight status of the child incorrectly more frequently in low-income households. Once more, these findings could be explained by the lower educational attainment of these parents and/or an increased prevalence of obesity among them, which would make them less likely to perceive excess weight in their children as a problem.26
The direct association between low household income and unhealthier dietary habits, in agreement with other studies conducted in Spain27 and at the international level,28 may be mediated by various mechanisms, such as poorer nutrition literacy in relation to a lower educational attainment, financial difficulties that limit shopping choice (especially of fresh foods) or lacking the time to cook, which in turn are associated with an increased consumption of precooked or processed foods, which have poorer nutrient profiles.29,30
Physical activity and sedentary behaviour were also associated with socioeconomic status in our study. We also ought to highlight the observed gender gap: girls were less physically active than boys, even within the same income bracket. The causes of this double inequality are multiple, and chief among them are, on one hand, greater access to sports activities and facilities in higher-income areas31 and a greater awareness of exercise as a contributor to health in families with greater educational attainment32 and, on the other, a family environment that is more supportive of sports in households with male offspring.33
The greater presence of electronic devices in the rooms of schoolchildren in households of lower socioeconomic status has also been observed in neighbouring countries.34 Parental educational attainment, parental setting of screentime limits and parental screentime could explain the observed differences based on income level.35
Other factors that were not addressed in our study are also associated with household socioeconomic status and the risk of childhood obesity, such as family structure, understood as the number of members of the household and the relationship between them, with evidence of an increased risk of obesity in households with a single parent and households with a single child.36 Another aspect that has been explored in the literature that is also associated with socioeconomic status and whose prevalence is increasing in the paediatric population is the presence of mental health problems in the child.37
When it came to the school environment, our study found that income level was also related to the type of school attended by the child as well as the available facilities and services. Indeed, the availability and actual access to sports facilities in the school are among the factors that may contribute to the level of physical activity in school-aged children, since, for instance, the number of facilities devoted to sports and play in the school has been found to be directly associated with the level of light physical activity and inversely associated with sedentary behaviour.38
Based on the results of the study, schoolchildren from low-income households grow in household and school environments that increase the risk of obesity, giving rise to what is known as an obesogenic environment through the interaction of factors of a very diverse nature: parental excess weight, lack of breastfeeding, inaccurate perception of the child’s weight status by the parents, less healthy lifestyle habits in terms of nutrition, physical activity and sedentary behaviour, greater availability of electronic devices and a school environment lacking a kitchen of its own, extracurricular sports activities or indoor sports facilities. Our findings highlight the need to develop effective multicomponent interventions to decrease childhood obesity, a problem exacerbated by the double income and gender gap, on the different environments.
The current literature supports the effectiveness of some early interventions to address both childhood obesity and child poverty.39 In Spain, a recent study found a lower prevalence of childhood obesity in regions where more resources were devoted to public health interventions, although prevention policy tended to have a greater effect in middle- and high-income groups, thus reproducing existing health inequalities.40
To address the inequalities and barriers identified in the study, it would be advisable to implement strategies aimed at reducing the burden of the obesogenic environment, and schools can offer an optimal equalising mechanism to narrow the income and gender gaps. The most important strategies would be those aimed at promoting a healthy diet and physical activity and those aimed at strengthening parental knowledge and awareness, especially in the most disadvantaged environments, in addition to ongoing epidemiological surveillance of childhood obesity and its determinants, with a particular emphasis on inequities.
The main strength of the study was that the analysis with a sex-gender perspective of the data of the ALADINO study, conducted in a large sample with objective anthropometric measurements and collection of data on multiple factor associated with the schoolchildren, their family background and their school environment, allowing the study of the obesogenic environment as a whole. Among its limitations, we ought to highlight that the data collected through self-report questionnaires may be a source of information biases such as recall bias and that the cross-sectional design of the study precluded the establishment of causality in the identified associations.
ConclusionThe prevalences of both overweight and obesity in schoolchildren in Spain are inversely associated to household socioeconomic status. Several factors, such as dietary and physical activity habits, the family background and the school environment, are also strongly associated with family socioeconomic status and may act as mediators in the aforementioned association, and there are also relevant differences based on the sex of the child. Interventions aimed at this important public health problem must be prioritised and adapted taking into account the identified inequalities to ensure their implementation can reach all children and be equally effective regardless of their socioeconomic background.
FundingThe ALADINO 2019 study was funded by the Agencia Española de Seguridad Alimentaria y Nutrición, which carries rounds of the ALADINO study at regular intervals in the framework of the Childhood Obesity Surveillance Initiative of the WHO Regional Office for Europe.
Conflicts of interestThe authors have no conflicts of interest to declare.
The following is Supplementary data to this article:
