

It has been observed that health professionals have difficulty performing quality cardiopulmonary resuscitation (CPR). The aim of this study was to compare the quality of ventilations performed by Nursing students on an infant model using different methods (mouth-to-mouth-and-nose or bag-valve-mask).
Material and methodsA quasi-experimental cross-sectional study was performed that included 46 second-year Nursing students. Two quantitative 4-min tests of paediatric CPR were performed: (a) mouth-to-mouth-and-nose ventilations, and (b) ventilations with bag-valve-mask. A Resusci Baby QCPR Wireless SkillReporter® mannequin from Laerdal was used. The proportion of ventilations with adequate, excessive, and insufficient volume was recorded and analysed, as well as the overall quality of the CPR (ventilations and chest compressions).
ResultsThe students were able to give a higher number of ventilations with adequate volume using the mouth-to-mouth-and-nose method (55±22%) than with the bag-valve-mask (28±16%, p<.001). The overall quality of the CPR was also significantly higher when using the mouth-to-mouth-and-nose method (60±19 vs. 48±16%, p<.001).
ConclusionsMouth-to-mouth-and-nose ventilation method is more efficient than bag-valve-mask ventilations in CPR performed by nursing students with a simulated infant model.
Se ha observado que los profesionales sanitarios tienen dificultades para realizar maniobras de reanimación cardiopulmonar (RCP) de calidad. Nuestro objetivo ha sido comparar la calidad de las ventilaciones en un modelo de lactante según el método utilizado (boca a boca y nariz o bien bolsa autoinflable y mascarilla facial) por estudiantes de Enfermería.
Material y métodosEstudio cuasiexperimental de corte transversal que incluyó a 46 estudiantes de Enfermería de segundo curso. Se realizaron 2pruebas cuantitativas de RCP pediátrica de 4min: a) con ventilación boca a boca y nariz; b) con ventilación con bolsa autoinflable y mascarilla facial. Se utilizó un maniquí Resusci Baby QCPR Wireless SkillReporter® de Laerdal. Se registraron y analizaron los porcentajes de ventilaciones con volumen adecuado, excesivo e insuficiente, además de la calidad global de la RCP (ventilaciones y compresiones torácicas).
ResultadosLos estudiantes consiguieron dar más ventilaciones con volumen apropiado con el método boca a boca y nariz (55±22%) que con bolsa y mascarilla (28±16%; p<0,001). La calidad global de la RCP también fue significativamente superior cuando aplicaron el método boca a boca y nariz (60±19 vs. 48±16%; p<0,001).
ConclusionesLa ventilación boca a boca y nariz es más eficiente que la ventilación con bolsa autoinflable y mascarilla facial en la RCP realizada por estudiantes de Enfermería con un modelo simulado de lactante.
In-hospital paediatric cardiac arrest (CA) is associated with relatively high rates of survival (30%–50%) and favourable neurologic outcomes in 60%–90% of patients.1,2 However, out-of-hospital paediatric CA is associated with low survival and a high risk of severe neurologic sequelae in survivors.3–6 The data reported by the Resuscitation Outcomes Consortium (a registry of 11 sites that provide emergency services in the United States and Canada) show that survival in these cases is associated with age: 3.3% of infants aged less than 1 year, 9.1% of children (aged 1–11 years) and 8.9% of adolescents (12–19 years).7 Estimates of neurologically intact survival range between 3% and 17%.8–10
The main difference between paediatric and adult CA is that most cases of paediatric CA are of a respiratory origin, either due to respiratory disease, choking or drowning, due to which the 2015 guidelines for cardiopulmonary resuscitation (CPR) of the European Resuscitation Council11 and the American Heart Association12 emphasise the need to deliver high-quality rescue breaths during paediatric CPR.13 When using basic life support techniques, ventilation must be delivered with the mouth-to-mouth technique (in children) or the mouth-to-mouth and nose technique (in infants). Where equipment is available, it is recommended that the child be ventilated with a bag mask ventilation (BMV) system, using the correct mask size for their age. All health professionals should have the necessary skills to use this technique effectively.11,13
Research has evinced poor CPR technique in students14,15 as well as professionals16 in the health care field. Some of these studies found that ventilation technique was inadequate,17,18 with a negative impact on patient outcomes.18–21
To our knowledge, no studies published to date have reported data on the quality of ventilation during CPR in infants based on simulation models (using manikins), so our aim was to assess the quality of rescue breaths delivered by nursing students using this approach, comparing the two recommended methods for ventilation: mouth-to-mouth and nose (M-MN) and BMV.
Materials and methodsWe conducted a cross-sectional quasi-experimental controlled study in a simulation environment. We selected participants by convenience sampling (volunteers). The sample consisted of 46 second-year nursing students enrolled in the School of Nursing of the Universidad de Vigo at Pontevedra. All participants had been trained on infant CPR. They were trained with an infant manikin with a real-time feedback system that measured parameters of chest compression and ventilation quality. The theoretical and practical training lasted 4h and was delivered in small groups (6 students). The training included infant CPR, both basic and instrumental (with BMV). The inclusion criteria were: having received scores of at least 70% in adequate ventilation, adequate chest compression and overall CPR quality during training, and providing informed consent for the use of collected data. Participation was voluntary. The data were anonymised. We conducted this study in adherence to the ethical principles of the Declaration of Helsinki.
Training and measuring equipmentWe used the Resusci® Baby QCPR manikin with the SimPad operating platform and wireless SkillReporter™ software, version 1.6 (all from Laerdal, Stavanger, Norway), which provides data on the main CPR metrics. The SkillReporter™ system provides feedback on the volume of air delivered in each ventilation, compression rate and depth, chest release following each compression, correct hand position and the frequency and duration of interruptions (Fig. 1). We used the Easyred child® 500mL self-inflating bag13,22 attached to the round Ambu® face mask, size 0A, with an internal diameter of 37.7mm and an external diameter of 73.1mm. We configured the simulation target ranges based on the 2015 ERC recommendations for CPR in infants.12 The manufacturer has not specified the approximate age of the manikin used for simulation, so we used the growth charts of the World Health Organization23 to estimate it based on its anthropometric measurements, finding that they were equivalent to those of an infant aged 3 months and weighing approximately 5.5kg. For assessment of correct compressions, we set a correct range of 100–120compressions/min for the rate of compression of and a of 38–45mm for the depth of compression.11 We set the correct volume of ventilation as a range of 6–10mL/kg, with delivery of 35–55mL of air per breath.13,24

Participants were grouped in pairs and performed 2 CPR simulation tests, each lasting 4min: (A) with the M-MN technique and (B) with BMV. Compressions were always performed using the “encircling technique” (applying pressure with both thumbs), as recommended by the ERC when there are 2 rescuers.11 Participants started the test (participant 1: ventilations, participant 2: compressions) and switched roles at 2min (participant 1: compressions, participant 2: ventilations). We paired participants and assigned their initial role at random. Participants could not see the system's feedback during the tests. After each test, participants were asked to rate their own technique in ventilation and in CPR overall. The tool used for self-assessment was a visual analogue scale25 represented by a line measuring 10cm. We avoided the use of numbers since they could induce bias by their potential association with scores. We compared the self-perceived quality with the objective measure of quality provided by the simulator by means of percentages.
Variables under study and statistical analysisDemographic variables: age, weight, height and body mass index of participants. Ventilation variables: ventilations with adequate volume (AVVs) expressed as percentage of total ventilations, ventilations with excessive volume exceeding the set maximum (VEVs) as percentage of total, ventilations with insufficient volume below the set minimum (VIVs) as percentage of total, ventilations with air inflow (VAs) as percentage of total, and ventilations with no air inflow (VNAs) as percentage of total, ventilations per minute during the test (V/min) and mean ventilation volume during the test (mVV) expressed in mL. Compression variables: correct compressions (CCs), expressed as percentage of total compressions. Correct compression was defined as chest compressions with a depth of 38–45mm with full chest recoil following compression, delivered at an appropriate rate (100–120compressions/min) with correct hand position. Quality CPR variable (QCPR): percentage score based on the number of effective manoeuvres. We calculated it following the following formula: QCPR=([AVVs+CCs]/2). We defined quality CPR as a score of at least 70% correct cardiac compressions and ventilations.26 Variables on self-perceived quality of CPR: self-perceived ventilation quality (pVQ) as percentage, and self-perceived CPR quality (pQCPR) as percentage.
We analysed the data using the software SPSS version 20 for Windows (SPSS; Chicago, IL, USA). We used the Shapiro–Wilk test to check the normality of variable distributions. We summarised variables using measures of central tendency (mean) and dispersion (SD) We performed comparisons by means of the Student t test for paired samples or a nonparametric test (Wilcoxon z) depending on whether the data followed a normal distribution. We defined statistical significance as a p-value of less than .05 in any of the tests. We calculated the effect size using the method proposed by Cohen or the one proposed by Rosenthal depending on whether the distribution was or not normal. We described the effect size using the categories proposed by Cohen27 and expanded by Rosenthal28: trivial (<0.2), small (0.2–0.5), moderate (0.5–0.8), large (0.8–1.3) and very large (>1.3).
ResultsThe 46 students included 10 men and 36 women. Their mean age was 23±6 years, and they had a mean height of 165±8cm, a mean weight of 67±12kg and a mean body mass index of 25±5kg/m2.
The percentage of ventilations that delivered an adequate volume was significantly greater using the M-MN technique. The percentage of ventilations that delivered an excessive volume was significantly greater with the BMV technique, while the percentage of ventilations that delivered an insufficient volume was significantly greater with the M-MN technique (Table 1). Participants perceived that they delivered higher-quality rescue breaths with the M-MN technique, but they rated their own technique in either method unfavourably (Table 2).
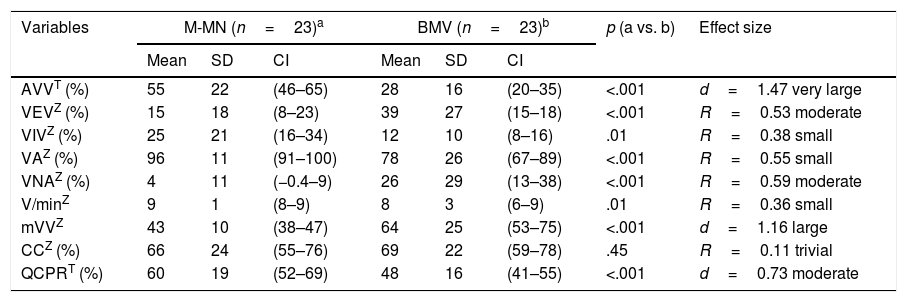
Results for the paediatric CPR variables.
| Variables | M-MN (n=23)a | BMV (n=23)b | p (a vs. b) | Effect size | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | CI | Mean | SD | CI | |||
| AVVT (%) | 55 | 22 | (46–65) | 28 | 16 | (20–35) | <.001 | d=1.47 very large |
| VEVZ (%) | 15 | 18 | (8–23) | 39 | 27 | (15–18) | <.001 | R=0.53 moderate |
| VIVZ (%) | 25 | 21 | (16–34) | 12 | 10 | (8–16) | .01 | R=0.38 small |
| VAZ (%) | 96 | 11 | (91–100) | 78 | 26 | (67–89) | <.001 | R=0.55 small |
| VNAZ (%) | 4 | 11 | (−0.4–9) | 26 | 29 | (13–38) | <.001 | R=0.59 moderate |
| V/minZ | 9 | 1 | (8–9) | 8 | 3 | (6–9) | .01 | R=0.36 small |
| mVVZ | 43 | 10 | (38–47) | 64 | 25 | (53–75) | <.001 | d=1.16 large |
| CCZ (%) | 66 | 24 | (55–76) | 69 | 22 | (59–78) | .45 | R=0.11 trivial |
| QCPRT (%) | 60 | 19 | (52–69) | 48 | 16 | (41–55) | <.001 | d=0.73 moderate |
AVV, ventilations that delivered adequate volume, as percentage; BMV, bag-mask ventilation; CC, correct compressions, expressed as percentage of total; CI, confidence interval; d, Cohen d for effect size; M-MN, mouth-to-mouth and nose; mVV, mean delivered volume during the test (in mL); p, p-value for an α level of 5%, established for all tests (p<.05); QCPR, quality CPR, expressed as percentage; SD, standard deviation; VA, ventilations with air inflow, as percentage; VEV, ventilations that delivered an excessive volume, as percentage; VIV, ventilations that delivered an insufficient volume, as percentage; VNA, ventilations with no air inflow, as percentage; V/min, ventilations per minute for the whole test.
We set the level of statistical significance at 5% for all tests (p<.05).
Effect size categories: trivial (<0.2); small (0.2–0.5); moderate (0.5–0.8); large (0.8–1.3); very large (>1.3).
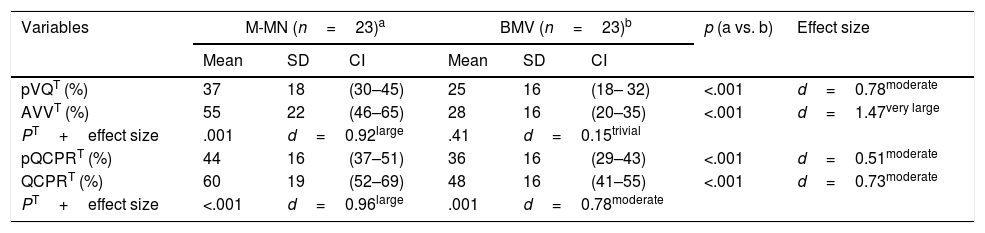
Participant self-rating of resuscitation skills.
| Variables | M-MN (n=23)a | BMV (n=23)b | p (a vs. b) | Effect size | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | CI | Mean | SD | CI | |||
| pVQT (%) | 37 | 18 | (30–45) | 25 | 16 | (18– 32) | <.001 | d=0.78moderate |
| AVVT (%) | 55 | 22 | (46–65) | 28 | 16 | (20–35) | <.001 | d=1.47very large |
| PT+effect size | .001 | d=0.92large | .41 | d=0.15trivial | ||||
| pQCPRT (%) | 44 | 16 | (37–51) | 36 | 16 | (29–43) | <.001 | d=0.51moderate |
| QCPRT (%) | 60 | 19 | (52–69) | 48 | 16 | (41–55) | <.001 | d=0.73moderate |
| PT+effect size | <.001 | d=0.96large | .001 | d=0.78moderate | ||||
AVV, ventilations that delivered an adequate volume, expressed as percentage; BMV, bag-mast ventilation; CI, confidence interval; d, Cohen d for effect size; M-MN, mouth-to-mouth and nose; p, p-value (level of significance defined as p<.05); pQCPR, self-perceived quality of CPR, expressed as percentage; pVQ, self-perceived quality of ventilations, as percentage; QCPR, quality CPR, expressed as percentage; SD, standard deviation.
Effect size categories: trivial (<0.2); small (0.2–0.5); moderate (0.5–0.8); large (0.8–1.3); very large (>1.3).
The quality of CPR manoeuvres is an essential factor in the outcomes of CA victims. However, there is evidence that health professionals deliver CPR of insufficient quality,17,18 which suggests that this is an area in need of improvement. To date, studies on the quality of CPR have mainly focused on the quality of chest compressions. Our study contributes novel data on the ability of previously trained nursing students on providing quality ventilations during paediatric CPR. The most relevant finding was that ventilation by the M-MN method resulted in better ventilation quality compared to the use of BMV.
We applied an arbitrary threshold of 70%26 of CPR manoeuvres within the recommended ranges to define quality in CPR. Some authors have proposed a less stringent threshold for quality (50%),29 and had we applied it, our sample would have succeeded in passing the quality threshold using the M-MN method. In our study, the percentage of ventilations with adequate volume was low using either method, which was consistent with the findings of the few studies conducted on this subject, such as the study by Madden,14 who found that undergraduate nursing students scored lowest on the “ventilation volume” component of adult CPR.
We were surprised by the low quality of ventilation using the BMV method observed in our study, considering that the students had been previously trained in this technique and that BMV is considered essential in the management of critically ill children and paediatric emergencies. Khoury et al.30 reported similar findings, which they attributed to the difficulty of handling self-inflating bags and of achieving a good seal between the mask and the victim's face. If this is the case, training on instrumental ventilation should be reinforced when nursing students are taught to deliver CPR to infants and children.
One of the challenges in ventilation during CPR is that some of the ventilations fail to deliver air to the lungs, either due to incorrect head and neck positioning or to a poor seal between the rescuer's mouth or mask and the victim's face. In our study, students succeeded in delivering air to the lungs in most ventilations (96%) with the M-MN technique, compared to only 78% of ventilations with the BMV approach. These findings are similar to those of Adelborg et al.31 in a study that compared different ventilation methods (M-M vs. BMV vs. mouth-to-pocket mask) in adult CPR delivered by lifeguards.
During CPR, in addition to ensuring that air reaches the lungs, it is important to deliver normal volumes to the patient, as hypercapnia or hypocapnia are both associated with poor outcomes.32 In our study, the percentage of ventilations that delivered insufficient volumes, that is, with a risk of hypercapnia, was greater with the M-MN technique (25%) compared to BMV (12%), with suggests that instrumental ventilation may offer some advantages over basic ventilation.
Avoiding hyperventilation (which may result from delivery of excessive tidal volumes, an excessive rate of ventilation or both) is also important.13 In this regard, Arshid et al. found that the number of ventilations per minute was excessive (>20/min) in 90% of advanced paediatric life support simulations.17 Furthermore, a study by Aufderheide et al. found that professional rescuers consistently hyperventilated real-life patients (37±4ventilations/min, that is, more than double the recommended rate).20 Contrary to these observations, the students in our study delivered a number of ventilations per minute that was just shy of the minimum recommended by the ERC,33 with no statistically significant differences based on the method used for ventilation. However, the volume delivered in many ventilations was excessive (39%±27% with BMV and 15%±18% with the M-MN technique), which would pose a risk of barotrauma and volutrauma in real patients. Furthermore, studies in animals have demonstrated that excessive ventilation increases intrathoracic pressure and decreases perfusion, which are associated with decreased survival.19,20 In this sense, M-MN may be safer than instrumental ventilation.
Our results show that nursing students provided better ventilation (in a simulated model) with the M-MN technique, which was consistent with the findings of Lawrence et al.,34 who also reported that the M-M approach was most effective. Practice with experimental models and clinical experience could be determinants of effectiveness in the use of BMV. In a study conducted in prehospital personnel, Terndrup et al. found no differences between the M-M and the BMV techniques, although they used less stringent objective criteria for the assessment of ventilation quality.35
Compared to ventilation, students in our sample achieved scores that came closer to the 70% quality threshold in the compressions delivered to the infant manikin, consistent with the findings of other studies that compared different ventilation techniques31,36 or compression-ventilation ratios.37 As one would expect, when we combined ventilations and chest compressions, the overall CPR quality was greater with the M-MN technique compared to BMV, as occurred in the study by Arshid et al.,17 which underscores the importance of ventilatory support during CPR in infants and children overall.
One significant aspect to consider in the practical training of health professionals is the correct self-assessment of skills, as there is evidence that perceived skills do not necessarily match reality: individuals often overestimate their own skills.38,39 However, our students underestimated their skills, which may be explained by their age, their status as students and their lack or professional experience.
Taking into account that most cases of paediatric CA have a respiratory cause,33 ventilatory support is essential in paediatric CPR, whether basic or advanced.13 The ERC guidelines acknowledge this difference, and recommend that health professionals that manage children be given access to training and equipment to provide BMV,11 which has been proven a safe and effective technique for delivery of CPR of short duration.40 However, in light of our findings, this approach may not be the best for nursing students, unless they receive more thorough initial training and regular retraining.
Limitations of the studyManikins are used frequently for training and skill evaluation, but they do not reflect real-world experience accurately, so our results cannot be directly extrapolated to clinical practice. In any case, our experience suggests that ventilation is more challenging in actual infants compared to manikins, which needs to be taken into account when interpreting our findings. Specifically, the manikin used in our study is easier to ventilate than a real infant, since air hardly ever leaks into the gastrointestinal tract in the manikin, making nearly all the air go into the lungs, a factor that may have led us to overestimate the effectiveness of both the M-MN and the BMV approaches.
Motivational factors, which vary significantly between simulated scenarios and real-life situations, also limit the practical validity of our data. Another potential limitation is the duration of the simulation test used in the study, which was shorter than the usual duration of real-life CPR, as in the latter rescuer fatigue may have a significant impact on the quality of CPR manoeuvres.
ConclusionsWe found that M-MN was more effective than BMV with a face mask in CPR delivered by nursing students in a simulated infant CPR model. This should be taken into account for the purpose of improving practical training of future nurses.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Santos-Folgar M, Otero-Agra M, Fernández-Méndez F, Hermo-Gonzalo MT, Barcala-Furelos R, Rodríguez-Núñez A. Ventilación durante la reanimación cardiopulmonar en el lactante: ¿boca a boca y nariz o con bolsa autoinflable? Un estudio cuasiexperimental. An Pediatr (Barc). 2018;89:272–278.
