


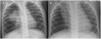


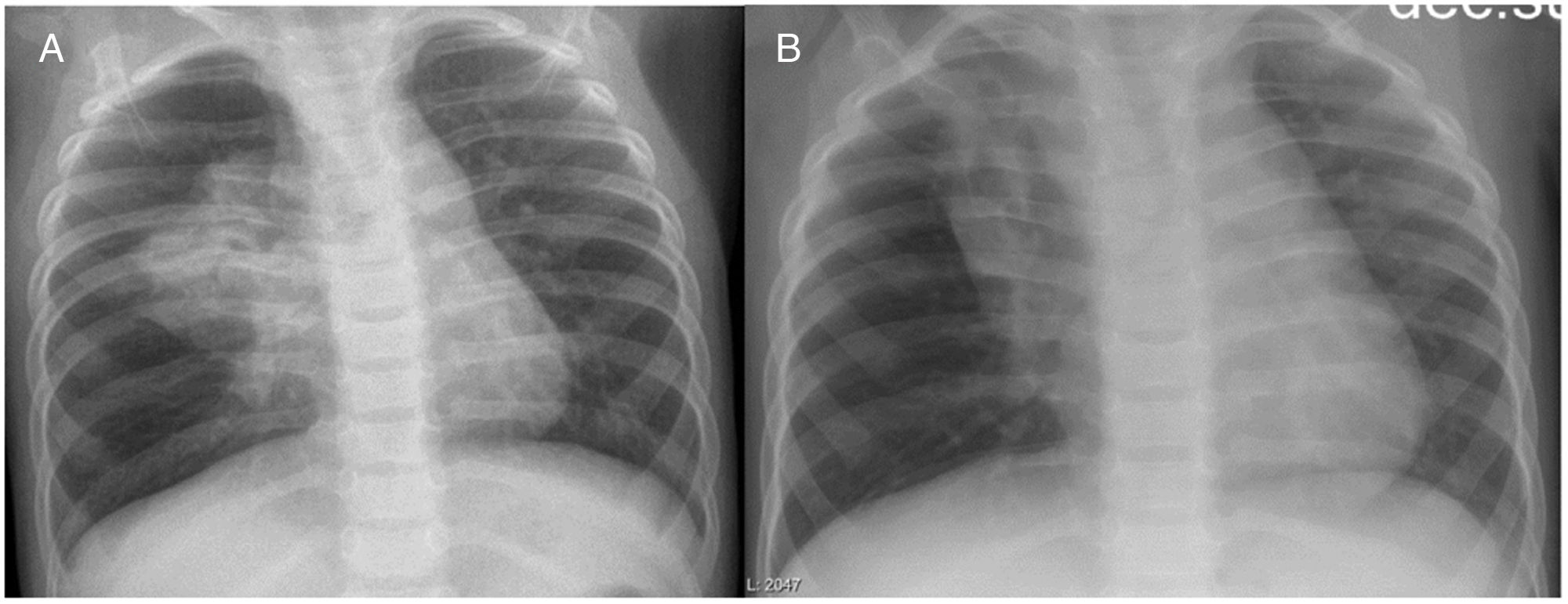
A girl aged 6 years with oculocutaneous albinism type 3 had pneumonia in the right upper lobe (RUL) of the lung at birth, and developed persistent infiltrate in the same location at a later time (Fig. 1). A computed tomography (CT) scan of the lung evinced partial atelectasis of the RUL with cystic bronchiectasis in the apical and anterior segments, right aortic arch and dilatation of the pulmonary artery (Fig. 2). Flexible bronchoscopy allowed the detection, near the carina, of a tracheal bronchus into which the bronchoscope could not advance due to collapse of the lumen, protrusion of the mucosa at the start of the right main bronchus and a decreased caliber of the opening to the RUL, with detection of two obliterated lumina (anterior and posterior segments) (Appendix A, Video 1).
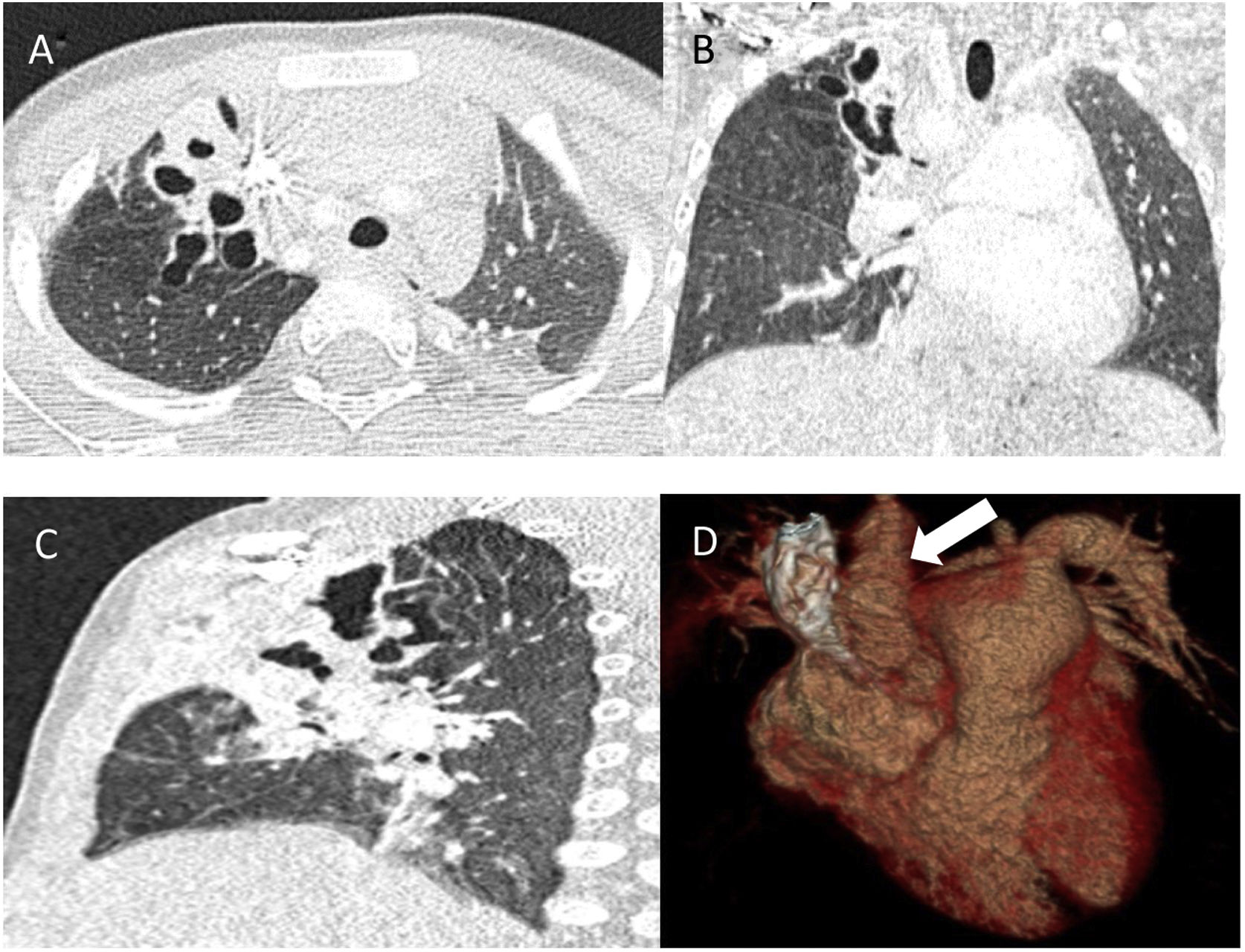
These findings suggested a tracheobronchial malformation due to the displacement of the apical segment of the RUL bronchus1 and the compression of this segment and the anterior segment by the aorta, with an abnormal right location, and development of bronchiectasis, which is not usually associated with tracheal bronchus.2,3 Due to the favourable clinical course, a conservative watchful waiting approach was decided on, and the patient is currently free of pulmonary infections. The follow-up CT scan 4 years later revealed residual retractile atelectasis with a fibrous appearance and bronchiectasis (Fig. 3).
Funding
This research did not receive any external funding.
