

Compliance with the recommendations regarding physical activity by adolescents is poor despite its proven benefits on their health.
ObjectiveThe objective of this study was to analyse the physical activity engagement in an adolescent population, evaluating its relationship with various indicators of physical and psychological health, as well as the influence of different sociodemographic variables as potential predictors.
MethodsA cross-sectional study was applied to a sample of 761 students (14.51 ± 1.63 years) from 25 schools in La Rioja (Spain). Physical activity engagement, hours of nightly sleep, maximum oxygen uptake, health-related quality of life, self-esteem, body image satisfaction, adherence to the Mediterranean diet, body mass index, academic performance and various sociodemographic factors were analysed for all participants.
ResultsBeing older, being a girl, having a low/medium socioeconomic level, living in unfavourable environments for practicing physical activity, not doing extracurricular sports activities, and being dissatisfied with body image were all predictors of a low physical activity engagement. Likewise, physical activity engagement reported positive associations with health-related quality of life, self-esteem, hours of nightly sleep, adherence to the Mediterranean diet and maximum oxygen uptake.
ConclusionsInterventions aimed at promoting physical activity must take into account these predictive factors, trying to favor their performance, especially in the most vulnerable groups.
El cumplimiento de las recomendaciones en torno a la actividad física por parte de los adolescentes es deficiente, a pesar de los demostrados beneficios sobre su salud.
ObjetivoEl objetivo del estudio fue analizar el nivel de actividad física en una población adolescente, evaluando su relación con diversos indicadores de salud física y psicológica, así como la influencia de diferentes variables sociodemográficas como potenciales factores predictores.
MétodosEl estudio se llevó a cabo sobre una muestra de 761 estudiantes (14,51 ± 1,63 años) de 25 centros educativos de La Rioja (España). Se valoró el nivel de actividad física, horas de sueño nocturno, consumo máximo de oxígeno, calidad de vida relacionada con la salud, autoestima, satisfacción con la imagen corporal, adherencia a la dieta mediterránea, índice de masa corporal, rendimiento académico y factores sociodemográficos de los participantes.
ResultadosTener mayor edad, ser chica, tener un nivel socioeconómico bajo/medio, residir en entornos desfavorables para la práctica de AF, no realizar actividades deportivas extraescolares y estar disconforme con la imagen corporal resultaron ser factores predictores de un nivel de actividad física bajo. Asimismo, la actividad física reportó asociaciones positivas con la calidad de vida relacionada con la salud, autoestima, horas de sueño nocturno, adherencia a la dieta mediterránea y el consumo máximo de oxígeno.
ConclusionesLas intervenciones dirigidas a la promoción de la actividad física deben tener en cuenta estos factores predictores, tratando de favorecer su consecución especialmente en los grupos más vulnerables.
Physical activity (PA) offers numerous demonstrated benefits throughout the lifespan. During adolescence, keeping an active lifestyle with inclusion of PA in the daily routine can prevent health problems.1 In consequence, the World Health Organization (WHO) recommends at least 60 min of moderate to vigorous PA for children and adolescents aged 5–17 years.2
The lack of PA seems to have a direct impact on body composition, with evidence of significant changes in the body fat percentage and the waist circumference,1 in as well as on body image and the self-concept.3 On the other hand, performance of PA has been found to have a beneficial effect on fitness, cardiovascular and metabolic health and different aspects of sleep.4 Furthermore, PA seems to also improve perceived quality of life and self-esteem, contributing directly to the prevention of different mental health disorders, such as depression or anxiety.5
However, despite the described benefits, regular practice of PA is inadequate in adolescents.6 In addition, the prevalence of sedentary lifestyles in this population is alarming and has become one of the greatest challenges in the field of health.7 In recent decades, the way leisure time is spent has changed significantly, with an increase in sedentary lifestyles to the detriment of PA, leading to changes in life habits and increased health risks.8 Thus, emphasis must be placed on the importance for health of childhood and adolescence, periods in which the development and consolidation of attitudes and habits related to PA are key for their maintenance during adulthood.9
The practice of PA seems to be based on different physical, psychological and sociodemographic factors.10,11 In this regard, the residential setting and school environment, social influence and the availability of activities and recreational and sports facilities also have a direct influence on the time spent by adolescents on PA.12
For this reason, knowledge of the predictors associated with PA in the adolescent population is particularly relevant, as it may be key in physical and psychological health prevention and promotion. Thus, in our study we analysed PA in a representative sample of adolescents and its association with different indicators of physical and psychological health, lifestyle habits, different sociodemographic variables and potential predictors. To do so, we assessed the level of PA, hours of night-time sleep, maximal oxygen consumption, health-related quality of life, self-esteem, body image satisfaction, adherence to the Mediterranean diet, body mass index, academic performance and several sociodemographic factors.
Material and methodsStudy design and participantsWe conducted a cross-sectional study in a sample of students enrolled in years 1 and 4 of secondary compulsory education (in Spanish, Educación Secundaria Obligatoria, or ESO) in schools in La Rioja, a region in northern Spain. We selected participants through single-stage cluster sampling, with the sampling units consisting of all classes of those 2 years in the region. To obtain a representative sample in both years and taking into account the total population (3470 students in year 1 of ESO and 2548 in year 4 of ESO), we calculated the sample size for a confidence level of 95% and a precision of 5% for an expected proportion of 50%. Based on these parameters, the sample would be representative with the inclusion of 346 year 1 and 334 year 4 students. Given that the mean number of students per class was 25 in both years, estimating a participation rate of 60%, we increased the figures just mentioned correspondingly, and then randomly selected 23 year 1 classes and 22 year 4 classes. All students in the selected classes were invited to participate in the study, and since 82% accepted, the final sample comprised 761 adolescents from 45 classes in 25 schools, 383 year 1 students and 378 year 4 students. Their ages ranged from 12 to 17 years (14.51 ± 1.63 years), and 49.7% were female and 50.3% male.
ProcedureWe requested the written informed consent of the parents or legal guardians of participants. Adolescents collaborated with the study on a voluntary basis after providing verbal assent. The study adhered to the ethical principles of the Declaration of Helsinki. The project was approved by the Clinical Research Ethics Committee of La Rioja. The data collection took place between January and June 2018.
InstrumentsWe estimated the level of PA by means of the Physical Activity Questionnaire for Adolescents, which has been validated in Spanish adolescents.13 The questionnaire assesses the PA performed in the past 7 days and has a score between 1 and 5 points, with higher scores reflecting more PA. We classified participants in tertiles based on the level of PA low, moderate, high. In addition, participants were asked about their participation in extracurricular athletic activities and the usual time they went to bed and woke up to calculate the duration of night-time sleep.
Cardiovascular fitness (CVF) was assessed with the Course-Navette test. Two lines were drawn across at a distance of 20 m to mark the beginning and end of the track. Participants had to run keeping time with beeps that determined the pace of traveling the distance between the 2 lines in succession. The initial running speed was 8.5 km/h, and it increased by 0.5 km/h each minute. The test ended when the participant stopped or failed to complete the distance at the set pace 2 consecutive times. Based on the results, we calculated the maximal oxygen consumption (VO2máx), using the formula provided by the author of the test.14
We estimated health-related quality of life (HRQoL) by means of the KIDSCREEN-27 questionnaire, validated in Spanish adolescents,15 which consists of 27 items rated on a Likert scale. We obtained the score following the directions of the authors of the questionnaire, and higher scores correspond to more positive perceptions of HRQoL.
We assessed self-esteem using the Rosenberg self-esteem scale, which has been validated in Spanish adolescents.16 It comprises ten items with answers scored on a scale from 1 to 4, with higher scores indicating greater self-esteem.
To assess the body image satisfaction, we used the method described by Stunkard and Stellar, validated in the Spanish population.17 It uses 9 female and 9 male figures that exhibit a progression toward a bulkier appearance, corresponding to different body mass index (BMI) values ranging from 17 to 33 kg/m2. Participants had to select 2 figures: the one with which they identified and the one they would like to have. Then, we calculated the difference between them, grouping the adolescents that were satisfied (values between −2 and 2) and those that were dissatisfied (all values outside the previous range) with their body image.
We assessed the adherence to the Mediterranean diet (MD) using the KIDMED questionnaire.18 The instrument includes 16 items with dichotomous answers (yes/no) regarding the consumption of foods associated with MD patterns. The overall score can range between −4 and 12, and higher scores indicate a greater adherence.
For the assessment of the environment for performance of PA, we used the ALPHA environmental questionnaire validated in the Spanish population.19 This questionnaire includes 10 items to assess the perception of aspects of the close environment (approximately in a 1.5 km a radius from the home) that may affect the engagement in PA. We categorized results applying the median as the cut-off point, defining 2 possible environments: favourable or unfavourable.
To detect and exclude from the analysis questionnaires completed at random, falsely or pseudorandomly, we used the Oviedo infrequency scale, a self-report instrument that includes questions with a basic dichotomous answer (yes/no).20 We inserted 6 items at different points in the questionnaire (for example, “Have you ever taken the bus?”). We excluded participants with more than 1 illogical answer from the analysis, specifically 2 of them.
When it came to sociodemographic data, participants reported their sex, date of birth and nationality (born in Spain or in a different country). We assessed socioeconomic status (SE) we administered the Family Affluence Scale (FAS II), which consists of 4 items that explore the material wealth of the family.21 The final score ranges between 0 and 9, and affluence is categorised as low (≤2), medium (3–5) or high (≥6). In the handling of the data, we combined low SES (1.8%) and middle SES (28%) into a single category due to the low frequency of the former.
To measure height and weight, we used a Holtain® stadiometer (Holtain Ltd, Dyfed, United Kingdom) accurate to 1 mm and a SECA® scale (713, Hamburg, Germany) accurate to 0.1 kg. Subsequently, we calculated the BMI and classified adolescents into normal weight, overweight and obesity categories based on the growth standards published by the WHO.22
Lastly, we assessed academic performance based on the grades provided by the Department of Education of the Government of La Rioja after obtaining the explicit consent of participating families, specifically of 90% of the total. We quantified performance by calculating the mean of the grades the student received the year that the study took place.
Statistical analysisWe have summarised quantitative variables as mean and standard deviation and qualitative variables as frequencies. We tested the normality of the data with the Kolmogorov-Smirnov test and the homogeneity of variance with the Levene test. We compared means using the Student t test in case of a normal distribution and otherwise the Mann–Whitney U test. We used the Pearson χ2 test to analyse the association of qualitative variables. To analyse the association between quantitative variables, we used the Pearson correlation coefficient in the case of a normal distribution and otherwise the Spearman correlation coefficient.
To identify potential predictors of PA and control for potential confounders, we conducted a multinomial logistic regression analysis. The “high PA level” group was the reference. We included the following variables in the model: sex, nationality, socioeconomic status, environment for performance of PA, extracurricular athletic activity, body composition and body image satisfaction. The statistical analysis was performed with the software IBM-SPSS®, version 25 for Windows (IBM Corp, Armonk, NY, USA). We defined statistical significance as a p-value of less than 0.05.
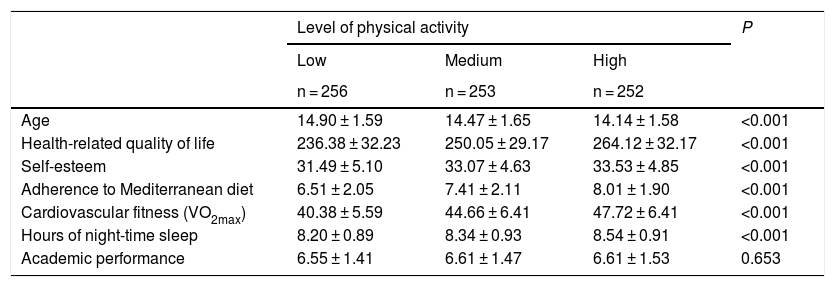
ResultsTable 1 presents the age, HRQoL, self-esteem, MD, VO2max, hours of night-time sleep and academic performance by level of PA in the adolescents under study. The analysis yielded significantly higher values in adolescents with higher levels of PA in all variables except for age, in which there was a significant but inverse association, and academic performance, in which we did not find significant differences based on PA.
Characteristics of the sample based on the level of physical activity.
| Level of physical activity | P | |||
|---|---|---|---|---|
| Low | Medium | High | ||
| n = 256 | n = 253 | n = 252 | ||
| Age | 14.90 ± 1.59 | 14.47 ± 1.65 | 14.14 ± 1.58 | <0.001 |
| Health-related quality of life | 236.38 ± 32.23 | 250.05 ± 29.17 | 264.12 ± 32.17 | <0.001 |
| Self-esteem | 31.49 ± 5.10 | 33.07 ± 4.63 | 33.53 ± 4.85 | <0.001 |
| Adherence to Mediterranean diet | 6.51 ± 2.05 | 7.41 ± 2.11 | 8.01 ± 1.90 | <0.001 |
| Cardiovascular fitness (VO2max) | 40.38 ± 5.59 | 44.66 ± 6.41 | 47.72 ± 6.41 | <0.001 |
| Hours of night-time sleep | 8.20 ± 0.89 | 8.34 ± 0.93 | 8.54 ± 0.91 | <0.001 |
| Academic performance | 6.55 ± 1.41 | 6.61 ± 1.47 | 6.61 ± 1.53 | 0.653 |
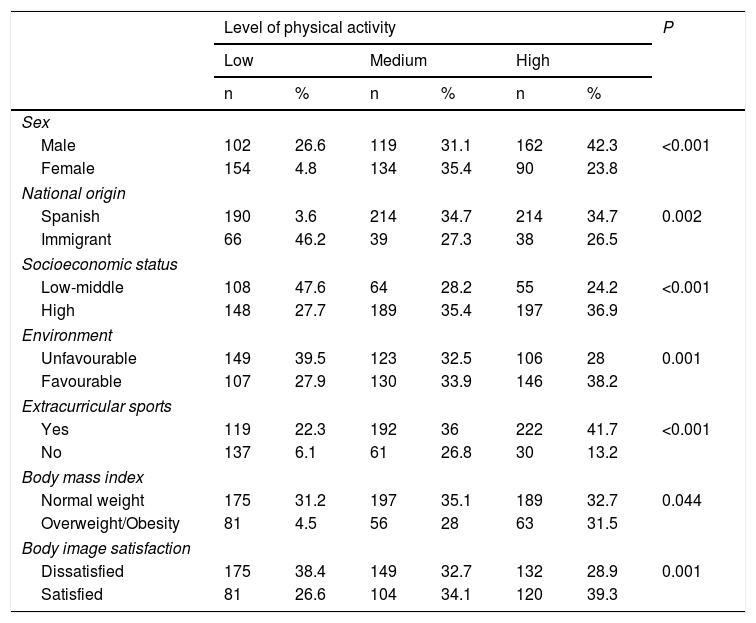
Table 2 summarises the results of the analysis of factors at play in the level of PA. We found lower levels of PA in students of immigrant origin, female sex, with a lower/middle SES, who resided in environments unfavourable for performance of PA, did not participate in extracurricular athletic activities, with overweight/obesity and dissatisfied with their body image.
Level of physical activity based on different factors.
| Level of physical activity | P | ||||||
|---|---|---|---|---|---|---|---|
| Low | Medium | High | |||||
| n | % | n | % | n | % | ||
| Sex | |||||||
| Male | 102 | 26.6 | 119 | 31.1 | 162 | 42.3 | <0.001 |
| Female | 154 | 4.8 | 134 | 35.4 | 90 | 23.8 | |
| National origin | |||||||
| Spanish | 190 | 3.6 | 214 | 34.7 | 214 | 34.7 | 0.002 |
| Immigrant | 66 | 46.2 | 39 | 27.3 | 38 | 26.5 | |
| Socioeconomic status | |||||||
| Low-middle | 108 | 47.6 | 64 | 28.2 | 55 | 24.2 | <0.001 |
| High | 148 | 27.7 | 189 | 35.4 | 197 | 36.9 | |
| Environment | |||||||
| Unfavourable | 149 | 39.5 | 123 | 32.5 | 106 | 28 | 0.001 |
| Favourable | 107 | 27.9 | 130 | 33.9 | 146 | 38.2 | |
| Extracurricular sports | |||||||
| Yes | 119 | 22.3 | 192 | 36 | 222 | 41.7 | <0.001 |
| No | 137 | 6.1 | 61 | 26.8 | 30 | 13.2 | |
| Body mass index | |||||||
| Normal weight | 175 | 31.2 | 197 | 35.1 | 189 | 32.7 | 0.044 |
| Overweight/Obesity | 81 | 4.5 | 56 | 28 | 63 | 31.5 | |
| Body image satisfaction | |||||||
| Dissatisfied | 175 | 38.4 | 149 | 32.7 | 132 | 28.9 | 0.001 |
| Satisfied | 81 | 26.6 | 104 | 34.1 | 120 | 39.3 | |
Table 3 presents the correlations between variables. In both sexes, the level of PA was positively associated with the hours of night-time sleep, HRQoL, self-esteem and the VO2max. In addition, 15.8% of the variance in the level of PA was explained by the HRQoL, 10.1% by the adherence to the MD and 3.8% by self-esteem.
Physical activity correlation coefficients.
| Health-related quality of life | Self-esteem | Hours of night-time sleep | Adherence to Mediterranean diet | Maximal oxygen consumption | |
|---|---|---|---|---|---|
| PA | 0.377** | 0.200** | 0.181** | 0.306** | 0.502** |
| PA, male | 0.421** | 0.253** | 0.146** | 0.329** | 0.399** |
| PA, female | 0.322** | 0.165** | 0.214** | 0.348** | 0.477** |
PA, physical activity.
*P < 0.05.
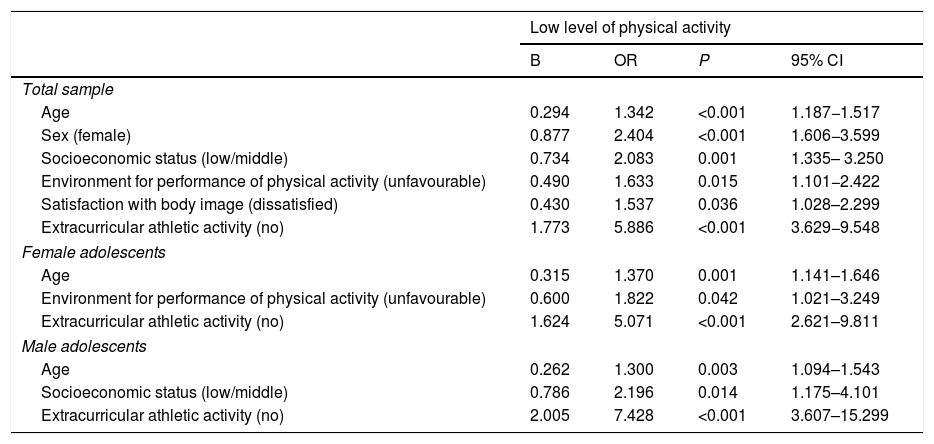
Table 4 presents the results of the multinomial logistic regression analysis with the high level of PA group as reference. It shows that the predictors of a low PA level were: lack of participation in extracurricular athletic activities, female sex, a low/middle SES, residing in environments unfavourable for PA and dissatisfaction with body image. When we considered predictors based on sex, we found that in both male and female adolescents, greater age and lack of participation in extracurricular sports activities were predictors of a low level of PA. In addition, residing in an environment unfavourable for PA was also a predictor in girls, while low/middle SES was a predictor in boys.
Factors associated with a low level of physical activity.
| Low level of physical activity | ||||
|---|---|---|---|---|
| B | OR | P | 95% CI | |
| Total sample | ||||
| Age | 0.294 | 1.342 | <0.001 | 1.187−1.517 |
| Sex (female) | 0.877 | 2.404 | <0.001 | 1.606−3.599 |
| Socioeconomic status (low/middle) | 0.734 | 2.083 | 0.001 | 1.335– 3.250 |
| Environment for performance of physical activity (unfavourable) | 0.490 | 1.633 | 0.015 | 1.101−2.422 |
| Satisfaction with body image (dissatisfied) | 0.430 | 1.537 | 0.036 | 1.028–2.299 |
| Extracurricular athletic activity (no) | 1.773 | 5.886 | <0.001 | 3.629−9.548 |
| Female adolescents | ||||
| Age | 0.315 | 1.370 | 0.001 | 1.141–1.646 |
| Environment for performance of physical activity (unfavourable) | 0.600 | 1.822 | 0.042 | 1.021–3.249 |
| Extracurricular athletic activity (no) | 1.624 | 5.071 | <0.001 | 2.621–9.811 |
| Male adolescents | ||||
| Age | 0.262 | 1.300 | 0.003 | 1.094–1.543 |
| Socioeconomic status (low/middle) | 0.786 | 2.196 | 0.014 | 1.175–4.101 |
| Extracurricular athletic activity (no) | 2.005 | 7.428 | <0.001 | 3.607–15.299 |
B, beta coefficient; CI, confidence interval; OR, odds ratio.
Note: we only present variables with P < 0.05.
Note: compared to “high level of physical activity” group.
Note: The reference categories were: sex (male = 1), socioeconomic status (high = 1), environment for physical activity (favourable = 1), extracurricular athletic activity (yes = 1), body composition (normal weight = 1) and satisfaction with body image (satisfied = 1).
The results of the study revealed an association between the level of PA and several sociodemographic variables, lifestyles and physical and mental health indicators, and we were able to identify a few predictors. One of them was sex, as female adolescents engaged in less PA and were twice as likely to have a low level of PA. The current literature supports that preferences, motivations and barriers for PA may differ between male and female adolescents.23 In this regard, a male-centred model of sports, in which available activities may not cover the needs of girls, could cause a lack of interest on PA during leisure time in this group.24 A systematic review of interventions for the promotion of PA in female adolescents25 highlighted the relevance of the educational setting and in particular of physical education, in which the creation of a pleasant atmosphere and the offering of a wide range of innovative activities of a mainly non-competitive nature, in addition to an increase in the number of hours devoted to the subject each week, could promote adherence with the recommendations on daily moderate to vigorous PA. Similarly, and given the influence of peers in this stage, the same review underscored the efficacy of strategies based on peer mentoring or leadership by specific classmates, in addition to the entire peer group. It also emphasised the need to implement global strategies with coordinated efforts by policy-makers and environmental and community agents, puberty as the ideal timing for their implementation and the need to acknowledge the different cultural practices and beliefs of girls of ethnic minorities.
Likewise, age was also found to be a predictor of PA, and a low level of PA was more likely to be found in older adolescents. This could be due to older adolescents spending more of their free time on sedentary activities (internet, videogames),26 the increased pressure in the context of sports, an increase in the time devoted to peers and heavier academic burdens.27
Also, engagement in extracurricular athletic activities was the strongest predictor of PA levels, and adolescents that did not participate in these activities were more likely to have a low level of PA. A study of adolescents in Europe revealed that those that participated in extracurricular sports were more likely to meet PA guidelines.28 When it came to this aspect, we found that 70% of the sample participated in these activities, a proportion similar to the one reported in European adolescents, of 67.2%.5
On the other hand, SES also turned out to be a predictor of PA, and children with low/middle SES engaged less in PA and male adolescents in this group, more specifically, were twice as likely to have a low level of PA. Previous studies have found a lower number of daily steps and a greater time spent in sedentary activities in association with low SES.11 In this regard, the fees required to join gyms or sports clubs could be determinants in this outcome, as they are considered one of the main barriers for lower-income families.29 For instance, lowering the cost of accessing sports facilities and athletic resources through financial aid programme in the form of vouchers was found to increase engagement in PA and improve the fitness of adolescents with lesser economic resources.30 Furthermore, the competent governmental and social institutions are key, as they can facilitate access to parks, playgrounds and outdoor gyms in addition to improving safety, lighting and the walkability/bikeability of the streets.31 In agreement with this, residence in areas that were not conducive to PA had a negative impact on its practice and was a predictor of a low level of PA in the case of female adolescents. Access to recreational facilities, walkability and residential density seem to be positively associated with PA outside school hours,32 highlighting the crucial role of the near environment in the practice of PA.
Lastly, body image satisfaction was also a predictor of the level of PA, and adolescents dissatisfied with their body images were more likely to have a lower level of PA. In this regard, that dissatisfaction could be one of the barriers to the engagement on PA, which would partly explain the obtained results.33
In addition to the predictors already mentioned, we also found that PA was associated with other sociodemographic variables, physical and mental health indicators and lifestyle habits. Thus, adolescents of immigrant origin reported lower levels of PA. A study conducted in adolescents in Norway found an increased risk of physical inactivity in children from immigrant families (OR, 1.31), and identified a low level of parental education as a determinant.34 Other reasons may be related to the lower participation of immigrants in sports clubs.35
As regards physical health indicators, the prevalence of overweight or obesity was greater in adolescents with lower levels of PA. The literature has underscored the preventive role of PA in cardiovascular diseases, as it achieves significant changes in the body fat percentage, waist circumference, systolic blood pressure and cholesterol.1 In addition, CVF also decreased with decreasing level of PA. Thus, PA of vigorous intensity seems to have a positive impact on CVF and the reduction of body fat.36 When it came to mental health indicators, we found a higher HRQoL and self-esteem in adolescents with higher levels of PA. Adhering to the PA recommendations of the WHO seems to produce an improvement in perceived HRQoL, especially in physical, mental and social health.37 In addition, interventions involving aerobic activity have been found to have positive effects on general as well as educational, family and social self-esteem.38
Lastly, when it came to results concerning lifestyle habits, the MD and sleep duration, we found lower values in adolescents with a low level of PA. In relation to this, there is evidence of an association between an increased time spent in sedentary activities and less healthy dietary habits.8 Furthermore, engagement in PA for more than 3 h a week has been associated with healthier dietary habits, with an increase in the consumption of vegetables, fish, cereal and nuts.39 As for the hours of night-time sleep, regular PA seems to have a beneficial effect on the total duration, efficiency, quality and latency of sleep.40
One of the main strengths of our study is that the sample was representative of the population. In addition, it allowed us to determine the associations between PA and different lifestyle habits, sociodemographic variables and health indicators and to identify several predictors of a low level of PA. Still, there were also limitations to the study, as responses to questionnaires are subjective, so we contemplate the use of more objective instruments, like accelerometers, as a possible future improvement. Nevertheless, previous studies in similar populations have demonstrated the reliability and validity of the instruments used. On the other hand, the cross-sectional design of the study precluded the establishment of causal relationships based on our findings, and longitudinal studies are required to complement these results.
Older age, female sex, a low/middle SES, residing in environments unfavourable for PA, lack of engagement in extracurricular athletic activities and dissatisfaction with body image were predictors of a low level of PA. In addition, PA was positively associated with HRQoL, self-esteem, the duration of night-time sleep, the MD and the VO2max. Our findings highlight the importance of sociodemographic factors in PA. Given the influence that PA has on health, interventions aimed at promoting PA should contemplate these factors, adjusting to the taste and needs of female adolescents and facilitating access to athletic activities for the most vulnerable groups, especially those with lower SES or living in environments that are not conducive to PA. Similarly, the promotion of organised sports in schools and universities should be considered as an effective tool to increase PA in youth.
FundingThe study was partially funded by the Instituto de Estudios Riojanos (IER) of the government of La Rioja through Resolution no. 55/2018 of July 9, by which the administration of the IER awarded the 2018–2019 grants for scientific studies on subjects related to the region.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Boraita RJ, Ibort EG, Torres JMD, Alsina DA. Factores asociados a un bajo nivel de actividad física en adolescentes de la Rioja (España). An Pediatr (Barc). 2022;96:326–333.
