



The recent development of three-dimensional (3D) imaging techniques has led to new applications in the field of medicine. Scanners and image-processing software have both become more accessible and simpler, allowing their use outside the fields of engineering and industry.1
Surface imaging contributes very useful information for a variety of complaints in the paediatric age group and has the advantage of image acquisition taking only a few seconds, which is of vital importance in very young patients.2
The purpose of this letter is to present our initial experience with a handheld 3D scanner for assessment of chest wall deformities.
In our hospital, we have started to use the PocketScan™ scanner (Mantis Vision Inc.). It is an infrared light system that automatically triangulates the position of different points on a surface, generating a 3D shape. The device measures 12×6cm and weighs 250g, and it can be connected to a computer with a standard USB cable. Its image-processing software can refine the resulting images and take any measures the user requires. Its price is of approximately 3500 €, and the funding for its purchase came from a research grant.
In the framework of a project whose objective is to validate these instruments and extend their use to other specialities, we started to perform body surface scans in patients with pectus carinatum and pectus excavatum managed in the Paediatric Surgery Clinic after obtaining the informed consent of their parents. We also assess these patients by magnetic resonance imaging (MRI) restricted to the region of interest with the intention of validating the 3D imaging method using the MRI scans as reference once we have carried out a sufficient number of evaluations.
We have performed an initial analysis of our experience with the first 10 patients, which we summarise below.
The sample consisted of 10 children and adolescents aged 7 to 17 years, 7 male and 3 female. Seven patients had pectus excavatum and 3 had pectus carinatum. The malformation was mild in 6 patients, moderate in 2 and severe in 2. Four of the patients were undergoing conservative management of their malformation at the time of the analysis. In case of children with pectus carinatum, conservative management involved the use of a chest brace following the Calgary protocol, and in case of pectus excavatum, the use of the vacuum bell method as described by a research group based in Basel.3,4
The rest of the patients, either due to their age or due to the low severity of the deformity, were managed with postural interventions and specific exercises per the protocol of our hospital.
All the scans involved acquisition of images over 3 to 4s, thus capturing data during inspiration as well as expiration for future investigation. There were no problems during the scan in any case; the obtained images were good and all children, as well as their parents, expressed satisfaction with the test and considering that it had no disadvantages.
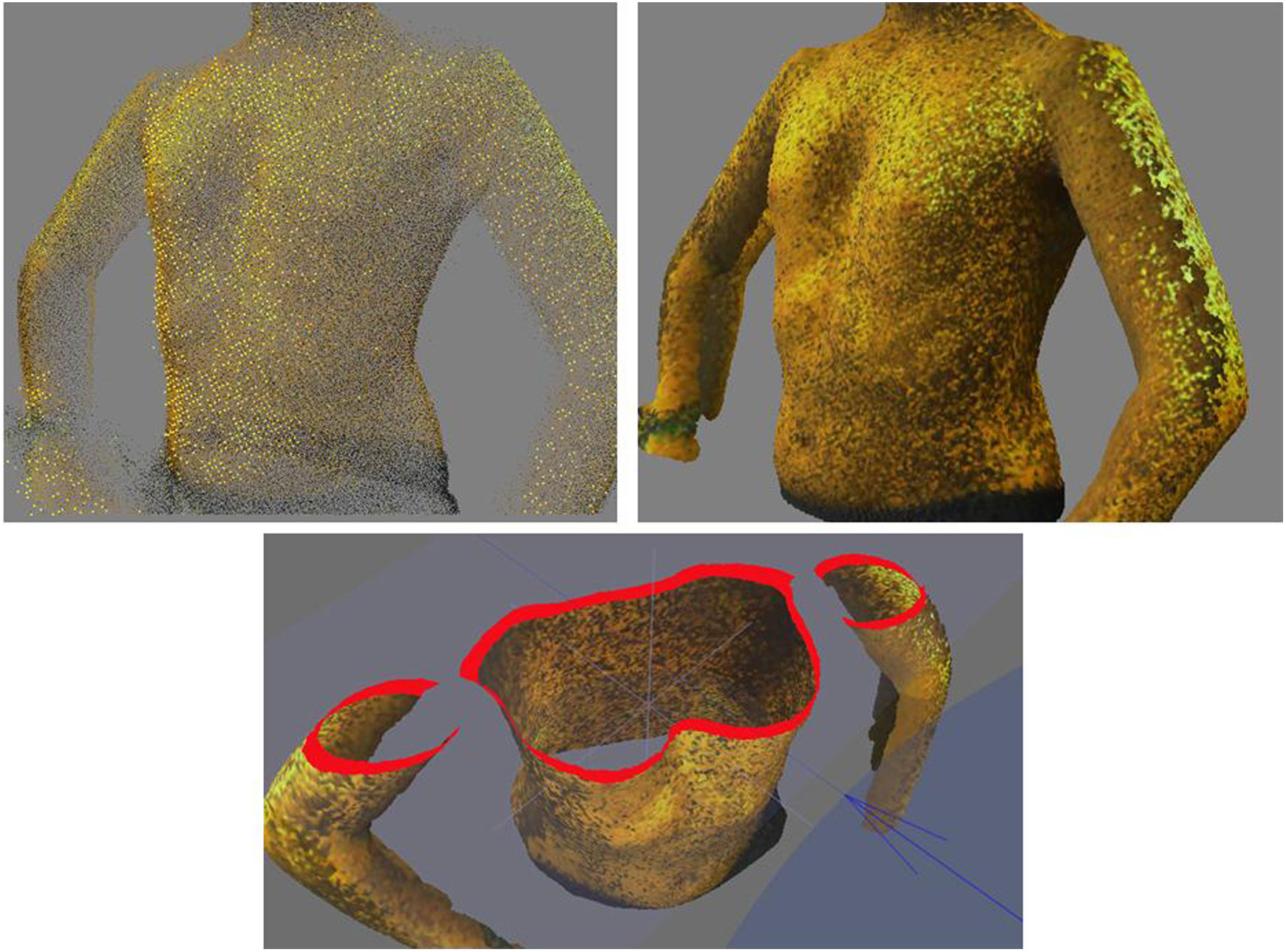
We exported the obtained 3D images for subsequent processing and to make specific measurements to determine the severity of chest wall deformity and to identify potential 3D measurements that could be useful for the diagnosis or definition of this type of problem (Fig. 1).
We consider our early experience with the 3D scanning system satisfactory, although we ought to admit that the image-processing software has not been developed with medicine in mind and thus health care professionals may need specific training to familiarise themselves with this system. The images obtained were highly accurate. The process for 3D image acquisition is fast and does not involve exposure to radiation, both of which we consider essential in paediatrics. Furthermore, compared to the subjective measures commonly used in clinical practice to assess these malformations, 3D scanning provides objective and accurate measurements. We also consider this essential in the follow-up of patients that are growing or undergoing conservative treatment to be able to detect changes over time or assess the response to different interventions. The cost of these devices is decreasing as this technology develops, making them more accessible to the public health care sector.
In conclusion, 3D scanning is a quick, radiation-free and accurate method, so it could have a broad range of applications in the field of paediatrics as a new tool in diagnostic imaging.
FundingResearch grant for funding of projects in biomedicine, health care management and social work and health care services. Regional Health Care Administration. Government of Castilla y Leon, 2017. Project file 1571/A/17).
Please cite this article as: Fuentes S, Damián F, Berlioz M, Pradillos JM, Lorenzo T, Experiencia inicial con el uso de un escáner tridimensional portátil. An Pediatr (Barc). 2020;92:236–237.
