



The transition to extrauterine life after birth has particular characteristics that call for a specific protocol for the neonatal stabilization and resuscitation in the delivery room. After the immediate postnatal period, although the precise temporal boundary has yet to be clearly established, there is controversy in regard to certain cardiopulmonary resuscitation manoeuvres in neonates, in which either neonatal resuscitation (NR) or advanced paediatric life support (APLS) recommendations may be applied. There are significant differences between them. For instance, the recommended ratio of chest compressions to rescue breaths (compression/ventilation ratio), of 3:1 versus 15:2, or whether chest compressions need to be synchronised with ventilation after endotracheal intubation, which results in decisions being made without sufficient evidence in support, ambiguous and arbitrary, which could pose risks to the safety of the patient. A review of the scientific literature, guidelines and manuals evinces a lack of consensus and as well as imprecision in the recommendations given by different scientific societies and working groups regarding the time at which the APLS guidelines should start to be applied instead of the NR guidelines, or whether the switch should happen at all.1–4 In the 3:1 compression/ventilation ratio, the cycle lasts 2s, so that 90 compressions and 30 breaths are delivered each minute. With the 15:2 ratio, which takes approximately 10s, 90 compressions and only 12 breaths are delivered in one minute. This difference is relevant due to the lower number of breaths delivered with the 15:2 ratio and its potential importance in relation to the probable cause of the need for resuscitation.
In Spain, there is no register of intrahospital cardiac arrest in neonatal patients, so there is no data on the current compression/ventilation ratios applied in newborns after the immediate postnatal period in real-world practice. For this reason, the Neonatal Resuscitation Group of the Sociedad Española de Neonatología (Spanish Society of Neonatology) designed a study to assess the management of cardiac arrest in neonates after the immediate postnatal period in relation to the application of NR or APLS guidelines.
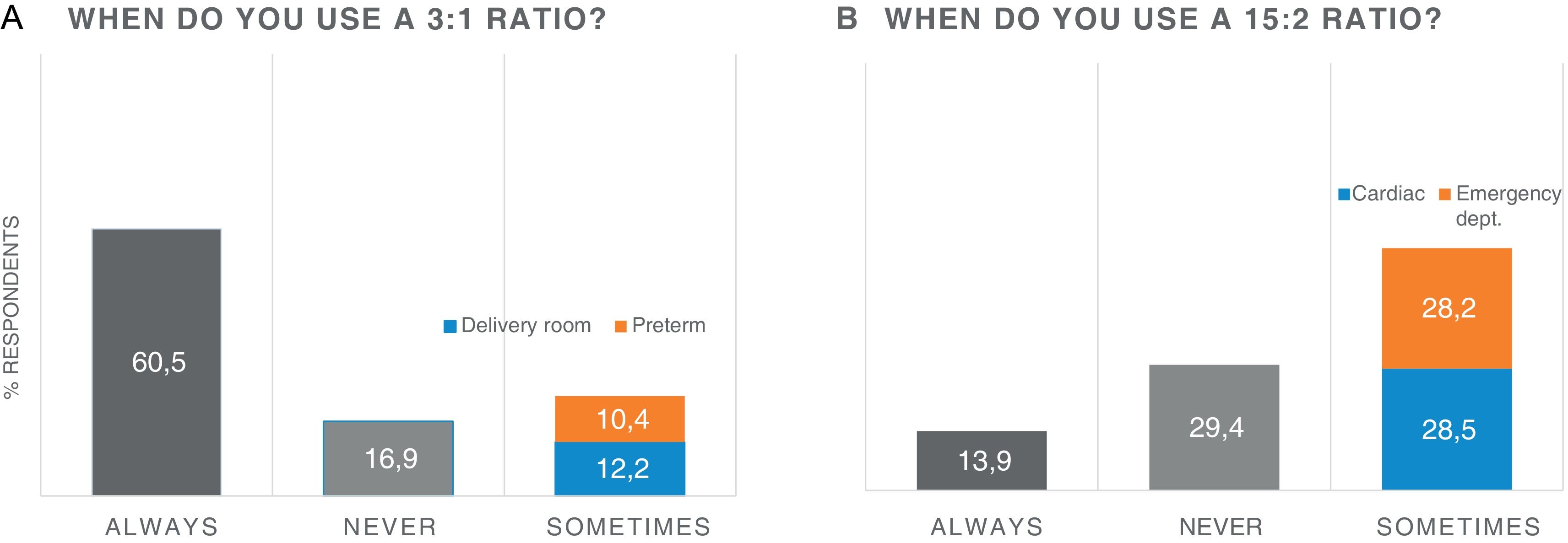
The study was conducted through a survey of neonatal units. Questionnaires were sent twice by electronic mail to the neonatologists members of the Sociedad Española de Neonatología who work in the public health system of Spain. It was submitted to 735 specialists, of who 307 (41.8%), employed in 114 centres, responded. Of these respondents, 82.4% (253) worked in a level III hospital, 13.4% (41) in a level II hospital and 4.2% (13) in a level I hospital. In addition, 67.7% (208) had more than 10 years of experience. Only 12 hospitals (10.5%) had a neonatal cardiac arrest management protocol for neonates outside the delivery room. When it came to the 3:1 compression/ventilation ratio, 60.5% of respondents reported using it always and 16.9% never using it. The remaining 22.6% reported that it depended on the setting (delivery room/maternity ward) and/or the gestational age (preterm or term newborn), as can be seen in Fig. 1. As for the 15:2 ratio, 13.9% of respondents used it in every case and 29.4% never used it. The remaining 56.7% reported that it depended on the probable aetiology (cardiac) and the setting (emergency care department) (Fig. 1b). In regard to chest compression and ventilation synchronization after intubation, 46.3% of respondents continued to synchronize them while 52.6% switched to unsynchronized chest compressions.
When it came to the care level, in level I and II hospitals the frequency of respondents who reported “always” applying the 3:1 ratio was lower (37.5%), with 20% reporting “never” applying it, with the percentage increasing to 40.5% among those who reported using it based on the setting (delivery room, maternity ward) or the gestational age. In level III hospitals, a higher proportion of providers reported “always” using the 3:1 ratio compared to level I and II hospitals (63.7%), while 16.5% reported never applying this ratio and 19.7% using it only based on whether the neonate was in the delivery room or maternity ward or the gestational age. That is, the 3:1 ratio was used more frequently in level III hospitals, while in level I and level II hospitals it was applied more frequently if cardiac arrest took place in the delivery room, in the maternity ward or in a preterm newborn.5
While we await further data, there continues to be a grey area in the management of neonatal patients, starting within minutes of birth, on which compression/ventilation ratio to apply. In the context of this controversy, it is providers who decide, individually or at the institutional level, which ratio to apply when the newborn experiences cardiac arrest outside the delivery room or the immediate postnatal period, with evidence of significant heterogeneity in the criteria used in decision-making in real-world practice, such as the aetiology, postmenstrual age and the setting where cardiac arrest occurs. We believe that there is an urgent need for specific recommendations for the management of neonatal cardiac arrest outside the delivery room.
