

We report the case of a boy aged 3 years presenting with fever, breathing difficulty and abdominal pain of 3 days’ duration and chronic constipation. His general health was adequate, he had polypnoea (50 bpm), an oxygen saturation of 98% and crepitus in the right lung base. The abdomen was soft, depressible and painless on palpation.
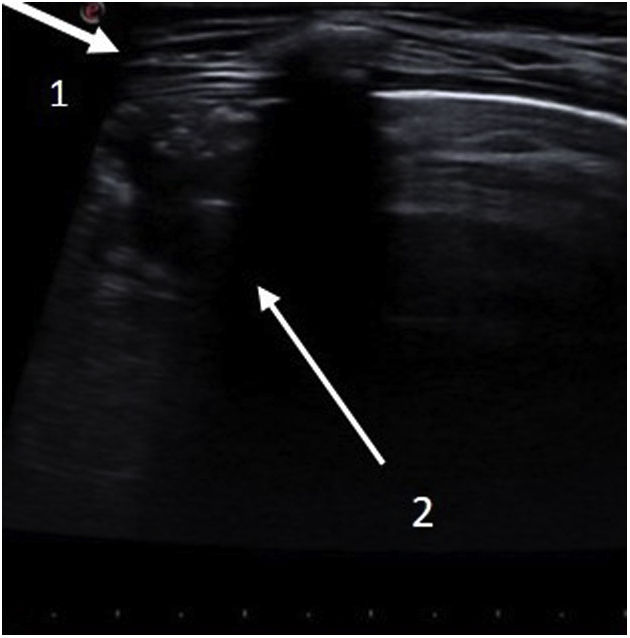
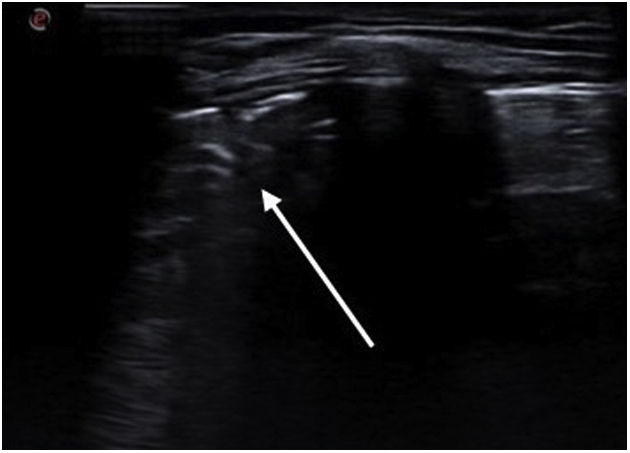
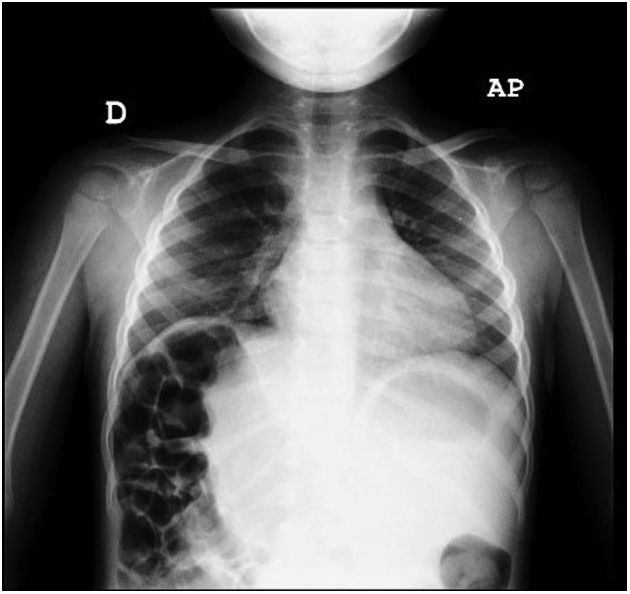
An ultrasound examination was performed due to suspicion of pneumonia (Appendix A, Video 1), evincing elevation of the diaphragm in the right hemithorax with subcostal interposition of bowel loops at the location of the liver and a small consolidation in the right middle lobe (Figs. 1 and 2). The radiographic features were suggestive of Chilaiditi syndrome (Fig. 3).
, with a consolidation pattern (arrow 2) and irregular margin (shred sign) occupying an intercostal space with a depth of 1.2 cm, compatible with incipient pneumonia.")
.")

The patient responded well to treatment with amoxicillin and macrogol, with resolution of symptoms and the liver found in its normal position in the follow-up ultrasound scan.
Chilaiditi syndrome is rare in children. Most cases are asymptomatic and are diagnosed due to a chance finding, in which case the condition is referred to as Chilaiditi sign. When the disease is symptomatic, patients present with breathing difficulty, vomiting, abdominal pain and constipation, and the condition is then referred to as Chilaiditi syndrome.
Conservative management with lifestyle and dietary measures and laxatives is usually effective. Surgical treatment is reserved for patients with severe complications, such as volvulus or other manifestations causing obstruction.
By presenting this case, we would like to highlight the value of ultrasound for both the diagnosis and follow-up of these patients.
The following is Supplementary data to this article:
Longitudinal plane at the level of the seventh rib. On the left there is a normal lung pattern with A-lines; at the centre, the curtain sign, and on the right (corresponding to the lower body), reverberation artefacts similar to A-lines. The pleura is not seen, which indicates that we are visualising a location in the abdominal cavity where we would normally find the liver. This should raise suspicion of Chilaiditi syndrome, in which intestinal loops are interposed between the diaphragm and the liver, displacing the latter.

