



Anterior uveitis is the most frequent type of uveitis in children1 and its diagnosis is usually delayed due to the difficulty of examining these patients.2,3
A boy aged 10 years presented with redness in the left eye of 3 weeks’ duration previously diagnosed as acute conjunctivitis and treated with topical gentamicin and dexamethasone without improvement. The patient sought care on account of the persistence of the problem, in addition to worsening epiphora, pain and photophobia.
The physical examination, which was challenging due to the lack of cooperation of the patient, revealed mixed injection (conjunctival and ciliary). There was no evidence of disruption of the continuity of the cornea with fluoresceine staining.
Since it was not possible to continue with the eye examination because the patient resisted eversion of the eyelids, we conducted an ocular ultrasound examination to rule out the presence of a foreign body and assess the structural and functional integrity of the eye. Both globes and optic nerves had normal morphology, size and sonographic appearance (Fig. 1), and the direct and consensual pupillary light reflexes (Figs. 2 and 3) were absent in the affected eye in comparison to the contralateral eye (Appendix A video).
. It is also useful to perform a transverse scan (Tran) to visualize the iris and pupil and assess the pupillary light reflex. A high-frequency (5–10MHz) linear probe is placed on the upper eyelid in the coronal plane at the level of the crystalline lens to visualize the iris, a structure surrounding an anechoic circular area that corresponds to the pupil. The images on top show both eyes in miosis upon the shining of a light through the eyelids. The “as low as reasonably achievable” (ALARA) approach must be applied to minimise thermal and mechanical indices. OD, right eye; OS, left eye.")
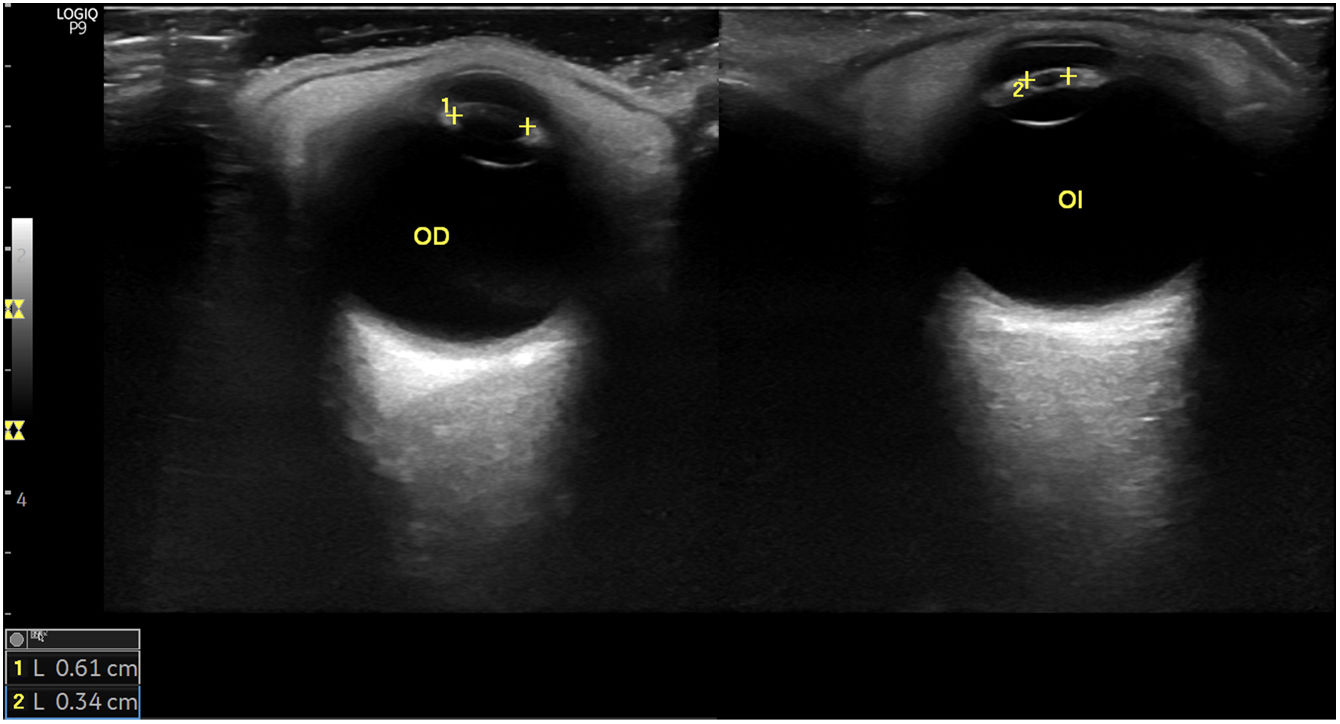
The ocular ultrasound examination is performed with the patient in the supine decubitus position with the eyes closed. At least 2 sagittal views should be obtained with the probe perpendicular to the horizontal meridian to visualize the globe and optic nerve (Sag). It is also useful to perform a transverse scan (Tran) to visualize the iris and pupil and assess the pupillary light reflex. A high-frequency (5–10MHz) linear probe is placed on the upper eyelid in the coronal plane at the level of the crystalline lens to visualize the iris, a structure surrounding an anechoic circular area that corresponds to the pupil. The images on top show both eyes in miosis upon the shining of a light through the eyelids. The “as low as reasonably achievable” (ALARA) approach must be applied to minimise thermal and mechanical indices. OD, right eye; OS, left eye.
 show the right eye in mydriasis due to the absence of light (assessment of direct and consensual reflex) and the left eye in miosis under the same conditions, evincing the absence of the pupillary light reflex, which was suggestive of inflammation in the anterior chamber (anterior uveitis). The images below provide diagrams of each of the images on top.")
The images on the top (Tran) show the right eye in mydriasis due to the absence of light (assessment of direct and consensual reflex) and the left eye in miosis under the same conditions, evincing the absence of the pupillary light reflex, which was suggestive of inflammation in the anterior chamber (anterior uveitis). The images below provide diagrams of each of the images on top.

The clinical features and the findings of the ultrasound scan, an inexpensive test that is quick and easy to perform by experienced providers, allowed the detection of a probable case of anterior uveitis (indirect diagnosis), so the patient was referred to the emergency department for an ophthalmological evaluation, where the diagnosis was confirmed by the slit-lamp examination.

