




Most cases of daytime incontinence in prepubertal girls have a functional aetiology, although a neurogenic dysfunction must always be ruled out. Vaginal reflux (VR) or intravaginal urination has been recognised as a cause of urinary incontinence with post void dribbling in prepubertal girls.1,2 The reverse flow of urine into the vagina can sometimes be perceived in a retrograde voiding cystourethrogram (VCUG), even in a standing position. This finding, which is frequent in prepubertal girls,1 may be asymptomatic or accompanied by symptoms such as diurnal incontinence and recurrent vulvovaginitis.3 Incontinence is characterised by loss of urine in the daytime (accompanied by enuresis in some cases) usually soon after urinating (post void dribbling) due to the progressive emptying of the vagina.1,3
We present 3 cases of VR that showed the usual clinical features of exclusively diurnal incontinence.
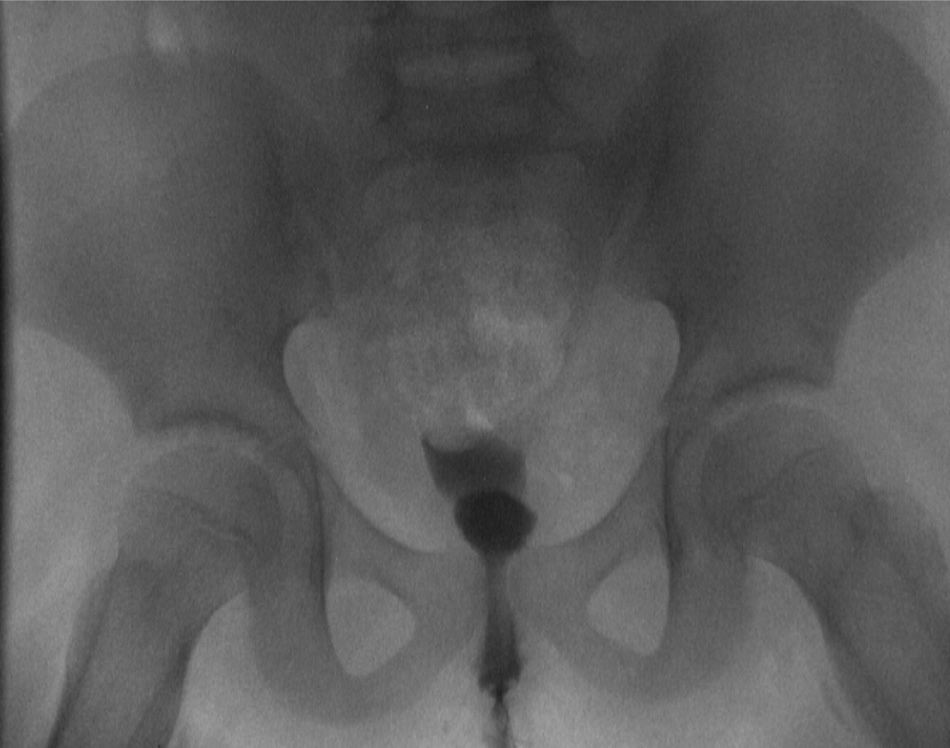
Case 1. Girl, 7 years of age, with overweight and symptoms of diurnal incontinence consisting of post void dribbling without enuresis. She reported occasional urgency and 3–4 episodes a year of afebrile urinary tract infection (UTI). We performed an ultrasound and a VCUG, with normal results. A uroflowmetry and urodynamic assessment were performed and showed no signs of pathology (coordinated urination without residual urine, no overactivity, correct voiding). Two filling cystometries were performed, the second of which (with the patient in a seated position) revealed a leakage that had not been detected in the first one. At first we considered the possibility of sphincter deficiency and we performed a magnetic resonance imaging study of the lumbosacral spine that showed no abnormalities. We reassessed the patient, reviewed the imaging tests, and found signs of VR in the VCUG (Fig. 1). This finding led to the prescription of urotherapy, and the symptoms resolved in 6 months.
Case 2. Girl, 9 years of age with diurnal incontinence and lower UTIs. She had received previous treatment with oxybutynin for suspected overactive bladder and showed no response to it. Uroflowmetry with electromyography revealed uncoordinated voiding, leading to the initiation of a biofeedback programme that had poor results despite improvement in the uroflowmetry tracings. It was decided to perform VCUG, which revealed VR (Fig. 2). Urotherapy specific to VR was initiated. Six months after starting treatment, the patient stopped having urine leaks.

Case 3. Girl, 7 years of age with sporadic dribbling and lower UTI. She had voiding postponement and decreased voiding frequency. Urotherapy was the only treatment prescribed. The patient did not show significant improvement by the following visit, so VCUG and ultrasound examinations were ordered, which revealed VR. There was evidence of low compliance with urotherapy, so we reinforced it with close monitoring by the nursing staff, stressing the importance of good toilet posture. The girl became asymptomatic after one year of followup.
Vaginal reflux may be the cause of incontinence in 12–15% of prepubertal girls with urine leakage.1,3–6 The diagnosis may be difficult if this possibility is not taken into account, requiring a multitude of diagnostic tests. It is common for voiding films taken during VCUG not to be examined in detail, as the emphasis is often placed on ruling out anatomical anomalies of the bladder and vesicoureteral reflux, and some paediatric radiologists are not familiar enough with VR. A bladder diary along with a structured history-taking usually reveals a pattern of incontinence, typically diurnal, post void dribbling (5–10min after urination) of a small volume,3 but large enough to require changes of clothing or some form of protection (such as sanitary pads). The genital anatomy in VR is completely normal and urine reflux from the urinary meatus to the vagina occurs when the legs are not spread during urination, the labia majora pose a barrier to the free flow of urine from the meatus, forcing the urine to flow back into the vagina.2–6 The habit of keeping the legs closed when sitting in the toilet obstructs the free flow of urine. Another factor that contributes to this reverse flow is the more horizontal vagina of prepubertal girls. This pattern is common in girls with an overactive bladder and “crossed legs” and in obese patients, and may play a role in recurrent vulvovaginitis.3
Once intravaginal reflux is identified, the treatment is satisfying. It consists of a urotherapy programme based on frequent or scheduled voidings, every 3h, adapted to family and school life, with a correct toilet position spreading the legs and leaning forward, or straddled on the toilet in the position opposite to normal (facing the wall), devoting enough time to urination (one minute or “counting to sixty”),1–6 with double voiding to try to empty any residual urine.7
Please cite this article as: Fernandez Ibieta M, Zambudio Carmona G, Martinez Castaño I, Guirao Piñera MJ, Ruiz Jimenez JI. Reflujo vaginal: una causa olvidada de incontinencia diurna en niñas prepúberes. Ann Pediatr (Barc). 2015;83:55–56.
