




The aim of this study was to evaluate the knowledge of first aid (FA) of primary and pre-school teachers and the parents of children in these education stages.
MethodsA questionnaire already used in previous publications was employed and consisted of 4 sections: (1) general information; (2) assessment of FA knowledge; (3) questions about FA, and (4) attitudes about FA. The questionnaire was sent by e-mail in Google Forms format to different education centres of the Autonomous Community of Galicia. The centres were asked to send them to the school staff and parents of the pupils so that they could be completed.
ResultsA total of 470 questionnaires were analysed (177 teachers; 242 parents and 51 teachers with children). More than half (268, 57%) of the participants stated to have knowledge of FA. In the case of the school teachers, associations were found between having undertaken some kind of FA training and teaching these contents (P=.008). Only 4 participants were able to put in the correct order the steps of the basic life support sequence, and nobody answered correctly all the questions about cardiopulmonary resuscitation. More than 95% of the sample were in favour to include FA in the school curriculum and in the study plans of university degrees aimed to train school/high school teachers.
ConclusionsThe majority of teachers and parents had training in FA, although they did not respond correctly to the questions related to basic life support. The inclusion of these contents in school curricula would be recommendable, but it would require training of the teaching staff beforehand. The inclusion of these contents in university study plans should be a measure to take into account.
El objetivo de este estudio fue evaluar los conocimientos en primeros auxilios (PP. AA.) de profesorado de educación infantil y primaria y de progenitores de niños en estas etapas educativas.
MétodosSe utilizó un cuestionario ya usado en publicaciones previas compuesto por 4 secciones: 1) información general; 2) valoración de los conocimientos en PP. AA.; 3) preguntas sobre PP. AA., y 4) consideraciones sobre los PP. AA. El cuestionario fue enviado a diferentes centros educativos de la Comunidad Autónoma de Galicia vía correo electrónico en formato Google Formularios. Se les solicitaba a los centros que los enviasen al claustro de profesores y progenitores del alumnado para su cumplimentación.
ResultadosEl número total de cuestionarios analizados fue 470 (177 docentes; 242 progenitores; 51 docentes con hijos). Doscientos sesenta y ocho (57%) participantes afirmaron poseer conocimientos en PP. AA. En el caso de los docentes, se encontró asociación entre tener formación e impartir estos contenidos en el aula (p=0,008). Solamente 4 participantes supieron ordenar la secuencia de soporte vital básico y ninguno respondió correctamente a a todas las preguntas sobre reanimación cardiopulmonar. Más del 95% de la muestra consideraba necesario incluir formación en PP. AA. En el currículo escolar y en los planes de estudios de carreras destinadas a formar al profesorado.
ConclusionesLa mayoría de los docentes y progenitores tenían formación en PP. AA., aunque no supieron responder correctamente a preguntas relacionadas con el soporte vital básico. Sería recomendable la inclusión de estos contenidos en los currículos escolares, pero para ello sería preciso formar previamente al profesorado. La inclusión de estos contenidos en los planes de estudios universitarios debería ser una medida a tener en cuenta.
Training of citizens in contents related to first aid (FA) and basic life support (BLS) is considered an essential strategy to improve the outcome of out-of-hospital cardiac arrest (OHCA). In this sense, a chain of different initiatives implemented nationwide in Denmark has facilitated a significant increase in the survival of victims of OHCA between 2001 and 2010.1 One of these initiatives was the inclusion of BLS in the elementary school curriculum, which contributed to increasing the number of events in which a witness of OHCA initiated BLS.
Recently, an international initiative named Kids Save Lives has been launched, which promotes the inclusion of BLS training in the elementary education curriculum, providing a rationale in 6 key points.2 Briefly BLS education in the general population should not depend exclusively on voluntary trainings; it is known that school children are able to learn BLS; and the goal of establishing a sense of responsibility from an early age makes the school environment the ideal setting for teaching FA. The implementation of the Kids Save Lives statement, supported by the World Health Organisation, would contribute to consider FA and BLS, traditionally considered to belong in the scope of health care professionals, a general object of learning, such as to ride a bike.3
The inclusion of these contents in the elementary school curriculum raises several questions, such as the age at which schoolchildren can start learning about BLS and who should be delivering training on the subject.
In recent years, evidence has emerged that training in FA could start as early as in the early childhood education stage. Positive outcomes of learning have been reported in children in the second cycle of pre-school education (kindergarten/preschool: ages 3–6 years) in remembering emergency phone numbers, assessing consciousness and breathing, placing the victim in the lateral recovery position, giving correct information to emergency calls and the use of the automated external defibrillator (AED).4,5 In the case of cardiopulmonary resuscitation (RCP), it has been demonstrated that children aged 9 years can learn it,6 and that 12-14 years old children achieve a quality of resuscitation (chest compressions) comparable to adults, in association with their physical growth.7,8
Although historically it was assumed that FA and BLS should be taught by health professionals, recent studies have evinced that school teachers (with adequate training) may be the collective that is best suited to do it.9–11
In addition to teachers, parents of young children should also have a significant role in this endeavour in different ways: on one hand, the numerous accidents that occur at home 12 could be immediately managed by parents if they were properly trained; and on the other, there is evidence that training of relatives can be a source and a booster of BLS learning in children.13
Therefore, we conducted a study with the objective of assessing the FA knowledge of school teachers (pre-school and elementary school) and parents children in the corresponding age groups.
Materials and methodsStudy design and participantsParticipants were teachers of pre- and elementary school and the parents of children enrolled in these stages in the region of Galicia, Spain. To assess the knowledge, attitudes and perceptions on FA and BLS and their potential inclusion in the school curriculum, we used a questionnaire that had been used in previous studies.14 We submitted the questionnaire by electronic mail to the administrative department of 681 public schools in the Autonomous Community of Galicia (pre-school centres, elementary schools and schools that offered both cycles). In the message, we asked school administrators to distribute the questionnaire to every teacher and parent in the school.
InstrumentWe reformatted the questionnaire14 into a Google form to facilitate access to it for schools and families. After a brief introduction, the form included 4 sections to be completed by each participant:
- (1)
General information: sex, age and province of residence; teachers also had to specify the education stage that they taught, their years of experience, whether they were from tutors/homeroom teachers and whether they taught contents related to FA; parents had to specify the number of children they had and the education stage that they were currently enrolled in.
- (2)
Assessment of knowledge on FA: dichotomous variable about whether they had or had not received training on FA. In case they had, we asked them to rate their knowledge, when they had received it and the reasons that they pursued it. In case they had no training in FA, we asked the reasons why.
- (3)
Questions about FA: (a) whether they would know how to act in case they found an apparently lifeless child; if the answer was “yes”, the respondent had to order the BLS sequence (check safety; check response; open the airway; look, listen and fell for normal breathing; call the emergency medical services; start chest compressions); (b) whether they would know how to deliver CPR; if the answer was “yes”, the respondent had to answer questions regarding the compression:ventilation ratio and the depth and rate of compressions in infants and children; (c) whether they knew what an AED is, and (d) whether they would know how to respond to foreign body airway obstruction (FBAO), and, should the answer be “yes”, to order the sequence (encourage to cough give back blows; give abdominal thrusts CPR).
- (4)
Attitudes and perceptions on FA and the possible inclusion on related contents in educational curricula: respondents were asked about which groups in the population they considered should be trained on FA, whether they believed it should be a mandatory subject in the curricula of schools and whether it should also be included in university degrees aimed to train teachers.
In addition, in the questions about the BLS and the FBAO sequences, participants who answered that they would know how to act were asked, after ordering the sequences, whether they believed they had ordered them correctly.
Statistical analysisVariables are shown as absolute and relative frequencies or as measures of central tendency (mean) and dispersion (standard deviation) as appropiate. We used the chi square test to compare independent groups. We defined statistical significance for all tests as a P-value of less than 0.05. We performed the statistical analysis with the statistical package IBM SPSS Statistics version 21 for Macintosh.
ResultsWe received 475 responses, of which we excluded 5 because they were from respondents that were neither teachers nor parents, so the final sample included 470 questionnaires (177 teachers; 242 parents; 51 teachers that were also parents).
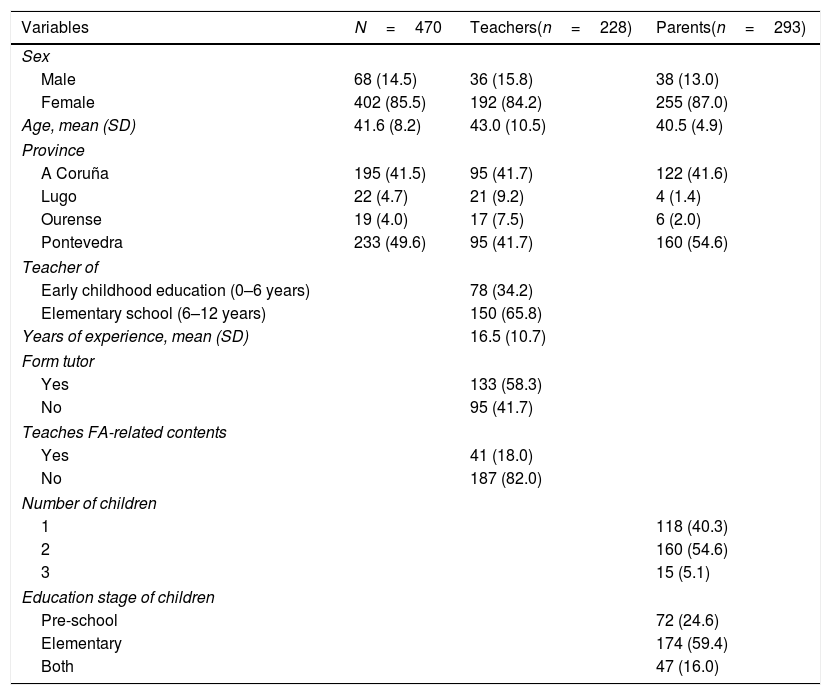
Respondent characteristicsTable 1 summarises the characteristics of the participants. We found a marked predominance of female participation (402 women; 85.5%) compared to male respondents. Forty-one (18%) teachers reported teaching FA-related contents. Of these teachers, 33 (80.5%) were form tutors, and we found a significant association between being a form tutor and teaching FA (χ2(1)=10.095, P=.001; Cramer's V=0.210, P=.001). We did not find an association between being a teacher as well as a parent and teaching FA-related contents.
Sample characteristics.
| Variables | N=470 | Teachers(n=228) | Parents(n=293) |
|---|---|---|---|
| Sex | |||
| Male | 68 (14.5) | 36 (15.8) | 38 (13.0) |
| Female | 402 (85.5) | 192 (84.2) | 255 (87.0) |
| Age, mean (SD) | 41.6 (8.2) | 43.0 (10.5) | 40.5 (4.9) |
| Province | |||
| A Coruña | 195 (41.5) | 95 (41.7) | 122 (41.6) |
| Lugo | 22 (4.7) | 21 (9.2) | 4 (1.4) |
| Ourense | 19 (4.0) | 17 (7.5) | 6 (2.0) |
| Pontevedra | 233 (49.6) | 95 (41.7) | 160 (54.6) |
| Teacher of | |||
| Early childhood education (0–6 years) | 78 (34.2) | ||
| Elementary school (6–12 years) | 150 (65.8) | ||
| Years of experience, mean (SD) | 16.5 (10.7) | ||
| Form tutor | |||
| Yes | 133 (58.3) | ||
| No | 95 (41.7) | ||
| Teaches FA-related contents | |||
| Yes | 41 (18.0) | ||
| No | 187 (82.0) | ||
| Number of children | |||
| 1 | 118 (40.3) | ||
| 2 | 160 (54.6) | ||
| 3 | 15 (5.1) | ||
| Education stage of children | |||
| Pre-school | 72 (24.6) | ||
| Elementary | 174 (59.4) | ||
| Both | 47 (16.0) | ||
FA, first aid; SD, standard deviation.
Data expressed as absolute (relative) frequencies unless noted otherwise.
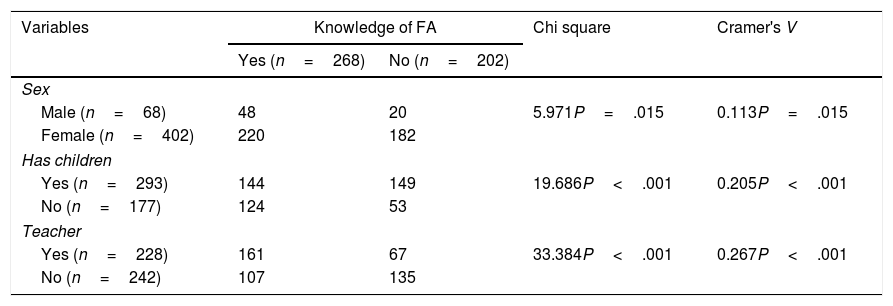
More than half of the participants (268; 57%) declared having some knowledge of FA. Table 2 presents the analysis of the association between having knowledge of FA and the independent variables under analysis. We found an association between sex and having knowledge of FA, with an overall greater proportion of males. However, we did not find a significant association with sex when we compared fathers vs mothers or male vs female teachers. We also found an association between having knowledge of FA and not having children and with being a teacher (P<.001 in both comparisons). In the specific case of teachers, teaching FA-related contents in the classroom was the sole variable that was positively correlated to having received training in FA (P=.008).
Association between knowledge of first aid in the sample and the independent variables.
| Variables | Knowledge of FA | Chi square | Cramer's V | |
|---|---|---|---|---|
| Yes (n=268) | No (n=202) | |||
| Sex | ||||
| Male (n=68) | 48 | 20 | 5.971P=.015 | 0.113P=.015 |
| Female (n=402) | 220 | 182 | ||
| Has children | ||||
| Yes (n=293) | 144 | 149 | 19.686P<.001 | 0.205P<.001 |
| No (n=177) | 124 | 53 | ||
| Teacher | ||||
| Yes (n=228) | 161 | 67 | 33.384P<.001 | 0.267P<.001 |
| No (n=242) | 107 | 135 | ||
| Variables | Only for teachers | Chi square | Cramer's V | |
|---|---|---|---|---|
| Yes (n=161) | No (n=67) | |||
| Teaches | ||||
| Pre-school (n=78) | 57 | 21 | 0.347P=.556 | – |
| Elementary school (n=150) | 104 | 46 | ||
| Form tutor | ||||
| Yes (n=133) | 98 | 35 | 1.450P=.229 | – |
| No (n=95) | 63 | 32 | ||
| Teaches FA | ||||
| Yes (n=41) | 36 | 5 | 7.119P=.008 | 0.177P=.008 |
| No (n=187) | 125 | 62 | ||
FA, first aid.
Of the 268 respondents that reported having knowledge of FA, 179 (66.8%) believed their knowledge was “acceptable”, and nearly half had had the last training more than 2 years before (133; 49.6%). Twenty-one described themselves as self-taught (7.8%). We did not find an association between the timing of training and the answers to the BLS questions.
The main reason why respondents reported taking trainings in FA is that they considered it essential knowledge (162; 60.4%). Most respondents with no previous training in FA reported they had not got any because they had never considered it (107; 53.0%), while 65 (32.2%) stated it was because they did not know where they could obtain such training (Supplemental Table 1).
Questions on basic life supportMore than half of respondents answered that they would know how to act if they found an unresponsive 6-year-old child (258; 54.9%), and this answer was positively correlated to reporting having knowledge of FA (χ2(1)=125.745, P<.001; Cramer's V=0.517, P<.001). However, only 4 respondents (1.6%) ordered the BLS sequence correctly. Of the 258 respondents that had stated they would know how to respond in this situation, 44 (17.1%) subsequently acknowledge that they did not know how to order the steps into the correct sequence.
Regarding CPR, 174 (37%) respondents declared being able to deliver it, an answer that was associated to having reported FA training: 165/174 (94.8%) (χ2(1)=161.136, P<.001; Cramer's V=0.586, P<.001). The questions regarding the compression:ventilation ratio and the depth and rate of compressions in a child aged 6 years were answered correctly by 33/174 (19.0%) and 17/174 (9.8%) of respondents, respectively. A total of 6 out of the 174 respondents (3.4%) answered both questions correctly. The results were similar when it came to infant CPR: 32/174 (18.4%) answered the compression:ventilation ratio question correctly, 9/174 (5.2%) the compression depth and rate question correctly, and 4/174 (2.3%) both correctly. None of the participants answered correctly all questions on child and infant CPR. We did not find a significant association between knowledge of FA and correct answering of any of the questions. We also found no significant associations between the condition of being a teacher, a parent or both and the results in the questionnaire to the questions on CPR.
As for the use of the AED, 396 respondents (84.3%) reported knowing its purpose, but only 55 (11.7%) reported knowing how to use it. Eight respondents (1.7%) acknowledged that they had never heard about AEDs.
In the case of FBAO, 286 participants (60.9%) answered that they would know what to do, of who 198 (69.2%) ordered the sequence correctly. Of those who answered they would know what to do, 60 (21.0%) subsequently acknowledged that they did not know how to order the steps in the sequence. We found a positive association between having knowledge of FA and correctly ordering the FBAO sequence (χ2(1)=7.949, P=.005; Cramer's V=.167, P=.005). As with CPR, we did not find a significant association between being a teacher, a parent or both and correctly ordering the sequence.
Supplemental Table 2 presents all the answers to the questions regarding BLS. Fig. 1 shows the percentage of participants, divided into parents (n=293) and teachers (n=228), that reported having knowledge of FA and responded correctly to questions on BLS. For comparison, it also includes the results of a previous study in future teachers.14

Percentage of participants that reported having had training in first aid and percentage of participants that responded questions about basic life support correctly. Comparison with a previous study in future teachers.14
Fig. 2 shows the opinions on which groups should have knowledge of FA, and Figs. 3 and 4 opinions on the inclusion of FA contents in the educational curricula of schools and of university degrees aimed to train future teachers, respectively. More than 80% of the sample considered that “everyone” should have basic knowledge of FA, and more than 95% of respondents considered that FA should be a mandatory subject in school and university curricula. Supplemental Table 3 presents the absolute and relative frequencies of the answers to these questions.
Discussion


Given the recommendation of training the general population in FA, it is necessary to establish “what the population knows” in order to identify “what it needs to learn” and determine “what” needs to be taught and “how”. This is one of the few studies that has attempted to assess knowledge of FA and the attitudes and perceptions of teachers and parents regarding its inclusion in school and university curricula.
In our study, with parents and schoolteachers of pre- and elementary school, we found a generalised lack of knowledge that was reflected in a majority of incorrect answers, specially in questions regarding BLS sequence and CPR. The fact that knowledge about FBAO is more widespread, or that this sequence is shorter than the sequence of BLS and involves steps that are less specific than CPR (respondents needed to know the correct depth and rate of compressions for both child and infant CPR), might explain the differences in knowledge observed between contents related to FBAO and all other contents. However, it seems that both teachers and parents were convinced that training on this subject should not be restricted to health care professionals or other collectives with the duty to act, and therefore that it should be a mandatory part of the curricula in lower and higher education.
Although there is ample evidence from multiple studies that bystander response to OHCA before the arrival of emergency services increases survival and improves outcomes, the fact is that in developed countries, the rates of bystander CPR, while slowly increasing, is very low.15 For years, intervention at the school level has been considered an ideal strategy to improve these statistics,16,17 as the school is the only setting that can reach the necessary percentage of the population (the critical mass) to achieve a significant increase in bystander response to any emergency,3,18,19 a percentage that could not be achieved by voluntary trainings or workshops.2,20
Taking these factors into account and that certain aspects of FA can be taught by the teaching staff in the framework of biology or physical education classes,9,20 these professionals should have the skills to teach these contents.
In our study, more than half of respondents reported having received some training in FA, similar to a study conducted in Belgium,21 but a greater proportion compared to studies in other countries: 50% in Turkey22 and 30% in Greece.23 Differences between countries in legislation may be one of the reasons that might explain these disparities. Based on the available data about the implementation of Kids Save Lives in Europe, in some countries, inclusion of FA training in the elementary school curriculum, in this case CPR, is mandatory, compared to other countries where it is an intervention to consider and other countries that have not officially stated an intent to implement such measures.24 Although more than half of the teachers and the parents had some training on FA, the answers to questions regarding BLS and FBAO were truly discouraging. These poor results could be explained by the fact that respondents had been trained more than 2 years ago. Although the effect of periodic trainings on emergency response skills is not a frequent variable under study,25 they are nevertheless recommended to prevent the loss of knowledge and skills.26
Despite the results obtained in the questionnaires, both teachers and parents considered that everybody should have knowledge of FA, with a discrepancy between the actual level of knowledge and the importance given to this knowledge that was consistent with the findings of previous studies.27 As mentioned above, achieving this goal would require the inclusion of FA contents in school curricula,20 something that respondents in our study and those of others of similar characteristics also considered necessary.14 This would lead to a general perception that acquiring this knowledge is the norm3 and would remove one of the main barriers involving bystanders in an emergency: doing nothing for fear of becoming the condition of the victim worse.28 However, the effective delivery of these educational contents in the school curriculum does not depend solely on the establishment of regulations on the subject; the mere inclusion of contents in the school curriculum does not entail that school teachers will be aware of them, and lack of training in teachers may also contribute to them not teaching this material due to not feeling qualified to do so.21 To remedy this lack of competence and increase the confidence of teachers requires instituting a national mandatory training programme on the subject,29 and a good strategy for the purpose would be to promote the inclusion of at least elective subjects on FA in the curricula of university degrees aimed to train future teachers (such as undergraduate degrees in pre-school education or elementary education), although ideally these would be mandatory core subjects. School teachers are the ideal collective to teach these contents, as knowing about FA is not the same as knowing how to teach FA,30 and teachers are the professionals knowledgeable about teaching strategies and methods. Both the teachers and parents in our study and future teachers that participated in a previous similar study14 considered such a measure necessary. Training teachers on FA would not only allow them to teach it to their students, but would also result in having a trained first respondent capable of acting in the potential event of an emergency in every classroom.
LimitationsThere are several limitations to our study. The response rate was low, which prevents the generalisation of results to the general population of teachers and parents. However, we consider that our results may be useful as an initial survey or pilot study for future studies with larger samples that could be compared to our own findings. In addition, the survey format cannot be used to assess the actual response skills of the participants. Also, since participants completed the survey at home or in the workplace, we had no way to ensure that they did not use any sources of information in the process. The questions that involved ordering a given sequence made answering easier compared to a question requesting the respondent to independently enumerate all the steps. Last of all, the questions that examined attitudes and perceptions carried a risk of response bias, as participants may answer what they consider may be perceived as “politically correct” rather than what they really think.
ConclusionsAlthough most of the teachers and parents that responded to the survey had received some training in FA, they did not know how to correctly answer questions concerning BLS. Both teachers and parents were in favour of including FA, BLS and FBAO contents in educational curricula. To reach this goal, as recommended by the World Health Organisation, the American Heart Association and European Resuscitation Council, it is necessary to previously train the teaching staff by including these contents in university curricula.
Conflicts of interestThe authors have no conflicts of interest to declare.
The following are the supplementary data to this article:
Please cite this article as: Abelairas-Gómez C, Carballo-Fazanes A, Martínez-Isasi S, López-García S, Rico-Díaz J, Rodríguez-Núñez A. Knowledge and attitudes on first aid and basic life support of pre- and elementary school teachers and parents. An Pediatr (Barc). 2020;92:268–276.
