

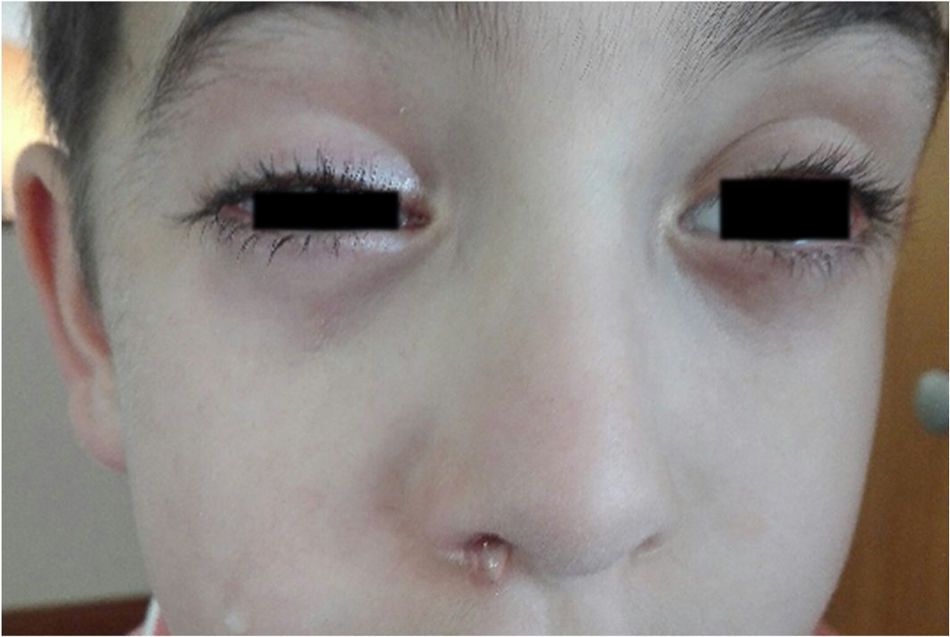
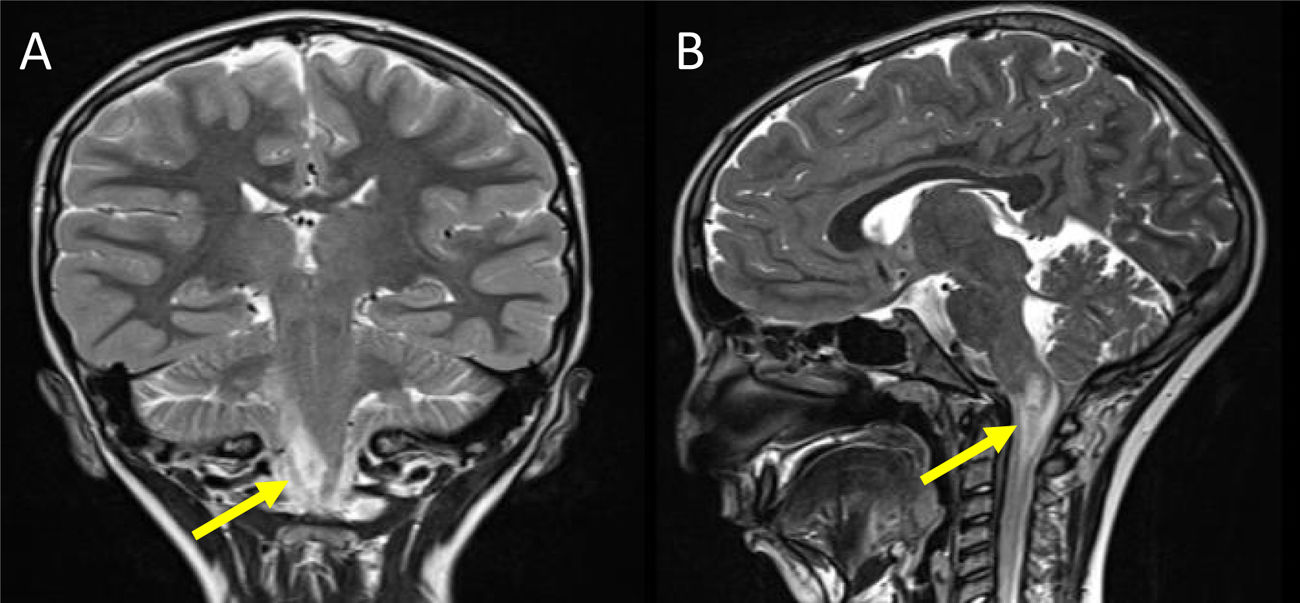
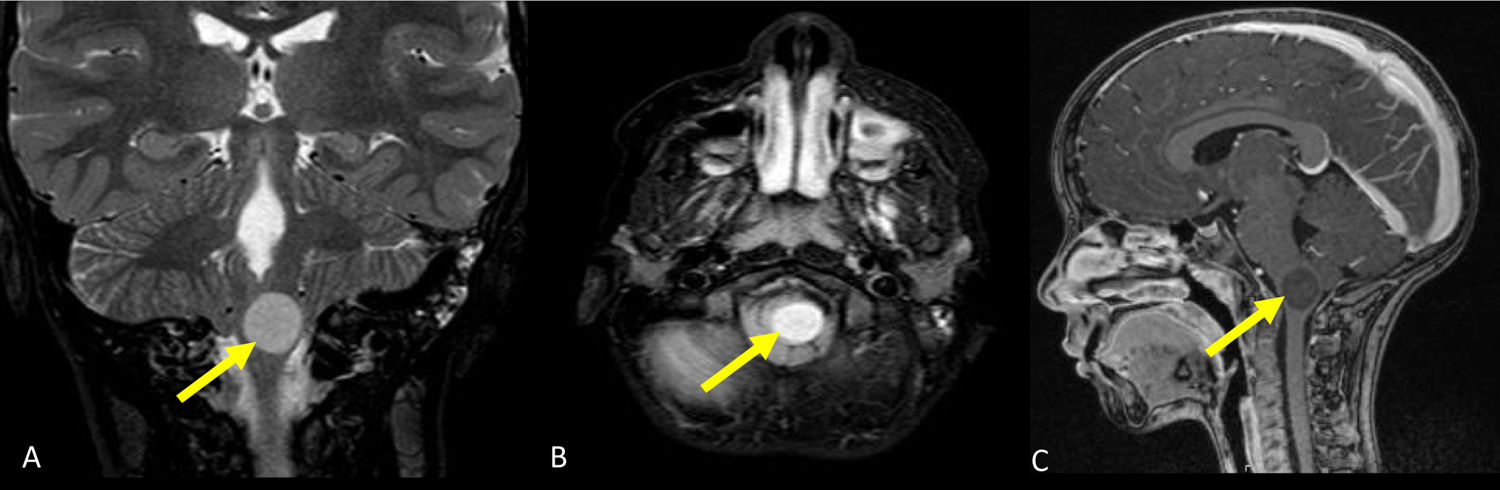
Trigeminal autonomic cephalalgias (TACs) are a group of infrequent primary headaches characterised by unilateral pain with trigeminal distribution associated with ipsilateral cranial autonomic symptoms, based on the definition of the International Headache Classification.1 Few cases have been described in the paediatric population, and lack of knowledge on the subject may result in misdiagnosis and delayed treatment. Much less frequently, an underlying lesion can cause symptoms like those of TAC, something that is not easily differentiated and whose recognition is of vital importance, as it may affect the treatment and outcome of the patient.2,3 In this article, we present two cases in boys aged 6 and 8 years, both with neurofibromatosis type 1 (NF1), who started to have recurrent short-lived unilateral headaches associated with ipsilateral autonomic features, such as conjunctival injection, lachrymation, ptosis and rhinorrhoea (Fig. 1). In both cases, the contrast-enhanced MRI scan detected the presence of pontomedullary low-grade gliomas (Figs. 2 and 3). The first one responded favourably to treatment with indomethacin, which, combined with the short duration of the episodes (<30minutes) led to a presumptive diagnosis of symptomatic chronic paroxysmal hemicrania. The second patient, who suffered cluster headaches lasting 2 to 3hours with a frequency ranging from every other day to eight times a day, was treated with chemotherapy, radiotherapy and surgical resection, and had a favourable outcome. These two cases illustrate that, although it is extremely rare, a “classical” presentation does not rule out the presence of an underlying disease causing the symptoms. Strictly speaking, the association of space-occupying lesions in the hypothalamic-pituitary region with TAC had already been described, but the cases we present underscore the important role that the trigeminal nucleus and trigeminovascular system may play in the pathophysiology of these headaches.4 Understanding and interpreting the underlying mechanisms requires knowledge of neuroanatomy, and the evaluation of any patient with a diagnosis of NF1 presenting with symptoms suggestive of TAC should include neuroimaging tests.
, unilateral and ipsilateral to the headaches.")
 involving the sensory nuclei of the trigeminal nerve (Case 1). (A) T2-weighted coronal view. (B) T2-weighted sagittal view.")
 involving the sensory nuclei of the trigeminal nerve, before and after gadolinium enhancement (case 2). (A) T2-weighted coronal view.(B) T2/FLAIR-weighted axial view. (C) Post-gadolinium T1-weighted sagittal view.")
Contrast-enhanced magnetic resonance imaging with showing a pontomedullary low-grade glioma on the left side (arrow) involving the sensory nuclei of the trigeminal nerve, before and after gadolinium enhancement (case 2). (A) T2-weighted coronal view.(B) T2/FLAIR-weighted axial view. (C) Post-gadolinium T1-weighted sagittal view.

