



Male adolescent aged 16 years with presenting complaint consisting of a 15-minute episode of loss of consciousness, facial and upper limb involuntary movements and urinary incontinence followed by excessive somnolence.
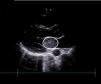
The findings of initial tests, including bloodwork, toxicology, head CT and lumbar puncture, were unremarkable. The patient then developed right-sided hemiparesis with homonymous hemianopia and aphasia (score of 9 on the Pediatric NIH Stroke Scale [PedNIHSS]). A cerebral CT angiogram revealed an embolic ischemic stroke resulting from the occlusion of the M2 segment of the left middle cerebral artery. The etiological evaluation revealed a large left atrial mass (Fig. 1), which was surgically excised and confirmed as a myxoma in the histological analysis.

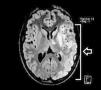
After surgery, the patient started treatment with aspirin (100 mg/day) and underwent structured motor and speech rehabilitation. Follow-up MRI scans (Figs. 2 and 3) showed stable ischemic lesions with no evidence of recurrent embolism. At present, the patient exhibits mild right hemiparesis, nominal aphasia (score of 5 on the PedNIHSS) and slight behavioral changes.


The management of pediatric stroke is challenging on account of atypical presentations and a broad differential diagnosis that includes seizures, migraine and vasculitis. Brain MRI is essential for accurate diagnosis. The role of reperfusion therapy, anticoagulation or antithrombotic strategies in children is unclear, given the limited evidence and lack of pediatric trials. Standardized protocols are essential for determining eligibility, guiding treatment and minimizing complications. This case highlights how performance of imaging and a comprehensive evaluation at an early stage is important to prevent recurrence and improve outcomes.1,2
